Short Answer
Short Answer
- Nerve hydrodissection is a non-surgical, ultrasound-guided procedure that uses fluid pressure to physically separate a trapped peripheral nerve from the tissue compressing it
- The injection delivers an injectate matched to the diagnosis (options include 5% dextrose, platelet-rich plasma, platelet lysate, protein concentrate (A2M), or autologous stem cells) in a 360-degree spread around the nerve under real-time ultrasound
- Most patients notice improvement within 2 to 3 months, with continued gains through 3 to 6 months and meaningful benefit often persisting at a year or longer in our clinical experience
If you have been dealing with burning, tingling, numbness, weakness, or sharp, aching, or diffuse pain that turns out to be coming from a trapped nerve, the pattern is usually the same. Physical therapy helped for a while. The brace or wrist splint took the edge off but never resolved it. The steroid injection worked for a few weeks, then the symptoms came back. You were told the next step is surgery, or that there is nothing more to do, or that the problem is "just nerve damage" you have to live with. The diagnostic workup never identified WHERE the nerve was being compressed, and no one offered a treatment that addressed the mechanical cause.
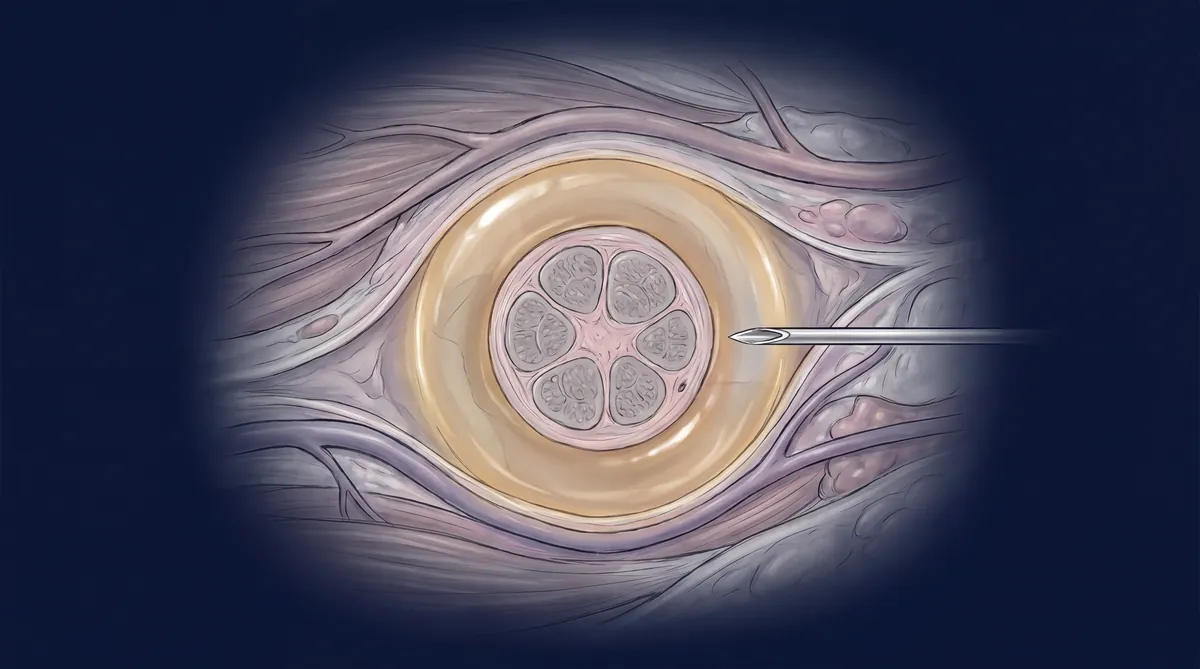
Nerve hydrodissection is a non-surgical injection procedure that uses fluid pressure, delivered under ultrasound guidance, to separate a compressed peripheral nerve from the surrounding fascia and scar tissue that has been entrapping it. It is performed in-clinic by physicians trained in musculoskeletal ultrasound, and it treats conditions like carpal tunnel syndrome, occipital neuralgia, meralgia paresthetica, cubital tunnel syndrome, and other peripheral nerve entrapments. Unlike nerve blocks that temporarily numb pain signals, hydrodissection physically frees the nerve and, when performed with platelet-rich plasma or other orthobiologics, delivers growth factors directly to the site of compression. Individual results may vary based on the severity and duration of the entrapment.
If conventional treatments have not given you lasting relief for your nerve pain, the next step is a detailed, in-person evaluation with diagnostic ultrasound to identify where the nerve is actually being compressed and whether hydrodissection is the right approach for your case.
Schedule a comprehensive 2-hour evaluation for your nerve pain at Regenerative Performance.
At Regenerative Performance, ultrasound-guided nerve hydrodissection is performed by physicians trained in musculoskeletal ultrasound, with Dr. Drew Timmermans holding RMSK (Registered Musculoskeletal Sonographer) certification. Every procedure starts with a full diagnostic ultrasound to identify the exact site of compression. The clinic performs advanced nerve hydrodissection with platelet-rich plasma and other autologous orthobiologics, not just dextrose or steroid.
Key Facts About Nerve Hydrodissection
Here is what you need to know about nerve hydrodissection before deciding whether it is worth exploring for your nerve pain.
- What nerve hydrodissection is: A non-surgical, ultrasound-guided injection technique that uses fluid pressure to physically separate a trapped peripheral nerve from the fascia and tissue compressing it, restoring normal nerve glide and delivering growth factors to the site of compression
- Who it helps: Adults with a clearly identifiable focal nerve entrapment (carpal tunnel, cubital tunnel, tarsal tunnel, occipital neuralgia, meralgia paresthetica, and other peripheral nerve compressions) who have not found lasting relief from medications, nerve blocks, bracing, or physical therapy. Patients with irritated or friction-stressed nerves (without true mechanical compression) often respond well too, and some entrapments are dynamic and only appear in certain positions on examination
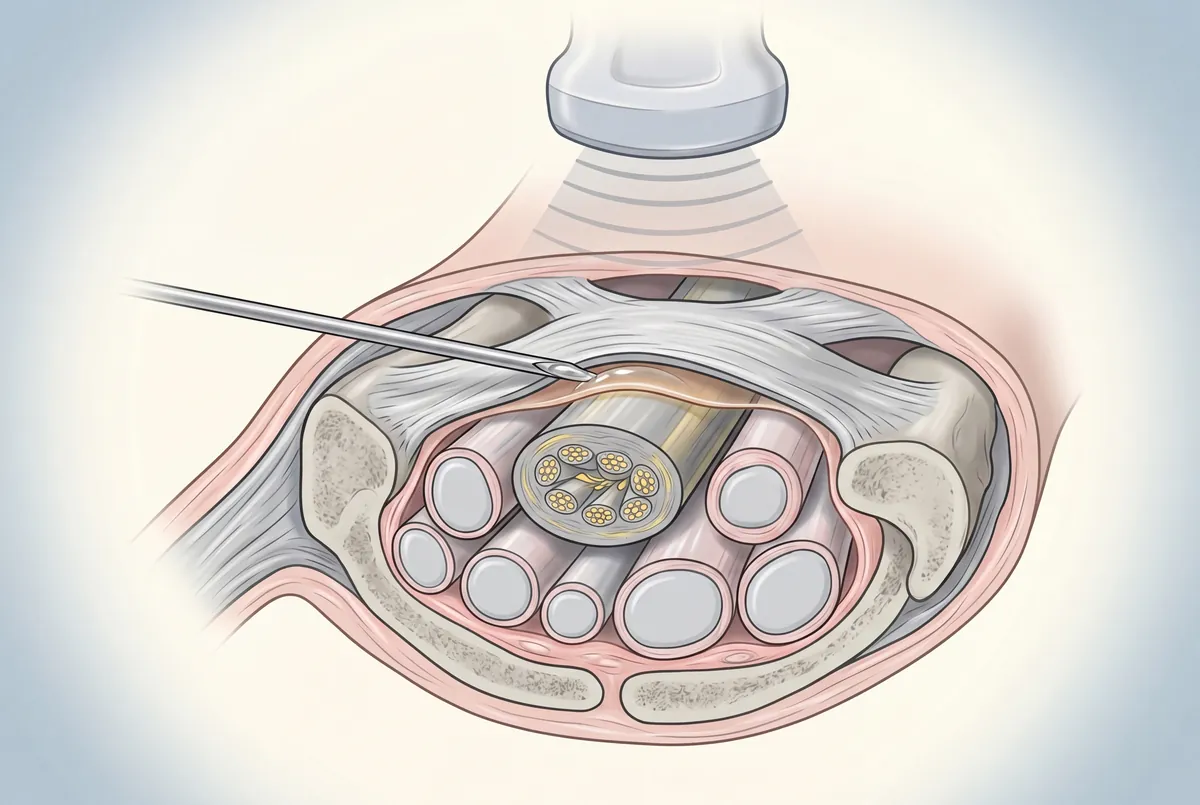
- How it works: Under real-time ultrasound guidance, a fine-gauge needle is advanced to the exact site of compression. Fluid (typically platelet-rich plasma combined with protein concentrate, layered with 5% dextrose) is injected to achieve 360-degree spread around the nerve, lifting the surrounding fascia and delivering platelet-derived growth factors directly to the nerve surface
- Goal of treatment: Mechanically free the nerve, restore normal nerve glide, reduce inflammation at the entrapment site, and support healing of the surrounding tissue
- Timeline: Most patients begin to notice changes within 2 to 3 months. Improvement typically continues building over 3 to 6 months, with meaningful benefit often persisting at a year or longer in our clinical experience. Individual results may vary
- Where: Regenerative Performance, a regenerative and interventional orthobiologic clinic in Gilbert, AZ
- Next step: Call 480-508-4226 to schedule a comprehensive evaluation
This guide is most useful if you have been diagnosed with a peripheral nerve entrapment, your nerve blocks or steroid injections wear off, and you want a non-surgical option that addresses the mechanical cause of the compression rather than only suppressing the pain signal.
What Is Nerve Hydrodissection and How Does It Work?
Nerve hydrodissection is a non-surgical procedure that uses the force of injected fluid to physically separate a peripheral nerve from the tissue that has been compressing it. The term "hydrodissection" literally means using water (hydro) to dissect or separate (dissection) tissue planes.
The procedure differs from a nerve block in several important ways. A nerve block injects anesthetic near a nerve to temporarily numb pain signals, with relief that lasts hours to days. Hydrodissection physically changes the relationship between the nerve and the tissue around it. The fluid creates a plane of separation, releases adhesions, and restores the nerve's ability to glide freely through its normal path. When performed with platelet-rich plasma or other autologous orthobiologics, the injected solution also delivers growth factors directly to the nerve surface, supporting healing of the surrounding tissue over the following weeks and months.
In a 2017 randomized controlled trial in Scientific Reports, Wu et al. found that a single perineural injection of platelet-rich plasma produced significant improvement in symptom severity, function, and median nerve cross-sectional area in patients with carpal tunnel syndrome, sustained at 6-month follow-up. A separate 2021 randomized trial in Archives of Physical Medicine and Rehabilitation by Chen et al. extended the follow-up to one year in moderate-to-severe carpal tunnel cases and found that PRP-treated wrists maintained meaningful improvement in symptoms, function, and electrodiagnostic measures at 12 months compared with the contralateral untreated wrist.
Why Does Nerve Entrapment Cause So Much Pain?
When a peripheral nerve becomes trapped, compressed, or adhered to surrounding fascia, the resulting symptoms can be disproportionate to what imaging shows. This is why so many nerve entrapment patients are told "everything looks fine on your MRI" while they are experiencing real, debilitating symptoms.
The conventional approach often jumps to nerve blocks or medications without identifying where the nerve is actually being compressed or what is causing the compression. The pain is real, the numbness and tingling are real, and the weakness is real. The problem is that the diagnostic approach often fails to pinpoint the mechanical cause.
Peripheral nerves need to glide freely through tissue planes as you move. When scar tissue, fascial thickening, or repetitive compression locks a nerve in place, several things happen at once. The nerve cannot slide normally during movement, which creates traction and irritation. Blood flow to the nerve decreases at the compression site, starving the nerve of oxygen. The nerve becomes hypersensitive, amplifying pain signals. Over time, the nerve can develop structural changes that make the entrapment self-perpetuating. Some of the proposed mechanisms behind hydrodissection's analgesic effect involve releasing compression on the small blood vessels and fine nerve branches that supply the nerve itself, restoring perfusion and reducing the inflammatory signaling that drives chronic neuropathic pain.
Treatments that only address the pain signal, such as medications, nerve blocks, or numbing injections, turn down the volume on the symptom without addressing the physical structure causing the problem. The nerve is still trapped when the medication wears off.
How Is Nerve Hydrodissection Performed?
The procedure typically takes 20 to 45 minutes depending on how many nerves are being treated and the complexity of the entrapment.
Ultrasound mapping. Before any injection, the provider uses diagnostic ultrasound to visualize the nerve along its course, identify the exact site of compression, and assess the surrounding tissue. The entrapment point is often not where the patient feels the most pain, which is why this step is non-negotiable.
Needle placement. Under real-time ultrasound guidance, a fine-gauge needle is advanced toward the entrapment site. On the screen, the provider sees the needle tip, the nerve, and the surrounding fascia simultaneously. This precision is what separates hydrodissection from a standard nerve block.
Fluid injection with 360-degree coverage. The goal is to ensure the fluid completely surrounds the nerve and releases the tissue around it. Full circumferential spread of fluid around the nerve is what determines whether the procedure achieves true decompression or only partially releases the surrounding fascia. Achieving that spread takes multiple needle redirections, small fluid boluses, and careful angle adjustments.
Following the nerve. Unlike a single-point injection, hydrodissection often follows the length of the nerve. The needle is repositioned multiple times to release the nerve along its entire course through the compressed area. This is one reason the procedure requires advanced ultrasound skills.
Biologic delivery. When platelet-rich plasma, platelet lysate, A2M, bone marrow concentrate, or microfragmented adipose tissue is used as the injectate, the growth factors and signaling molecules in those solutions come into direct contact with the nerve surface. The more surface contact between the injectate and the nerve, the more growth factor absorption occurs over the following 5 to 10 days. A 2019 head-to-head randomized trial in the Journal of Tissue Engineering and Regenerative Medicine by Shen et al. compared perineural PRP to perineural 5% dextrose for moderate carpal tunnel syndrome and found both produced meaningful 6-month improvement in symptoms and median nerve cross-sectional area, with PRP producing the greater reduction in median nerve cross-sectional area on follow-up imaging.
What Conditions Does Nerve Hydrodissection Treat?
Nerve hydrodissection works best for clearly identifiable, focal peripheral nerve entrapments. Here are the most common conditions treated.
Carpal tunnel syndrome. The median nerve becomes compressed by the transverse carpal ligament in the wrist. The PRP randomized-trial evidence at the median nerve is the strongest in the literature for any peripheral nerve hydrodissection application.
Cubital tunnel syndrome. The ulnar nerve becomes trapped at the elbow, causing numbness and tingling in the ring and pinky fingers. Hydrodissection releases the nerve from the surrounding fascia at the cubital tunnel.
Tarsal tunnel syndrome. The tibial nerve is compressed at the ankle, similar to carpal tunnel but in the foot. Symptoms include burning, tingling, and numbness in the sole of the foot.
Occipital neuralgia. The greater occipital nerve becomes entrapped at the back of the head, causing headaches that radiate from the base of the skull upward. A 2024 paper by Lam et al. in Diagnostics described novel ultrasound-guided hydrodissection techniques targeting the greater occipital nerve with 5% dextrose and reported clinical improvement in patients with occipital neuralgia where conventional treatments had provided only limited or temporary relief.
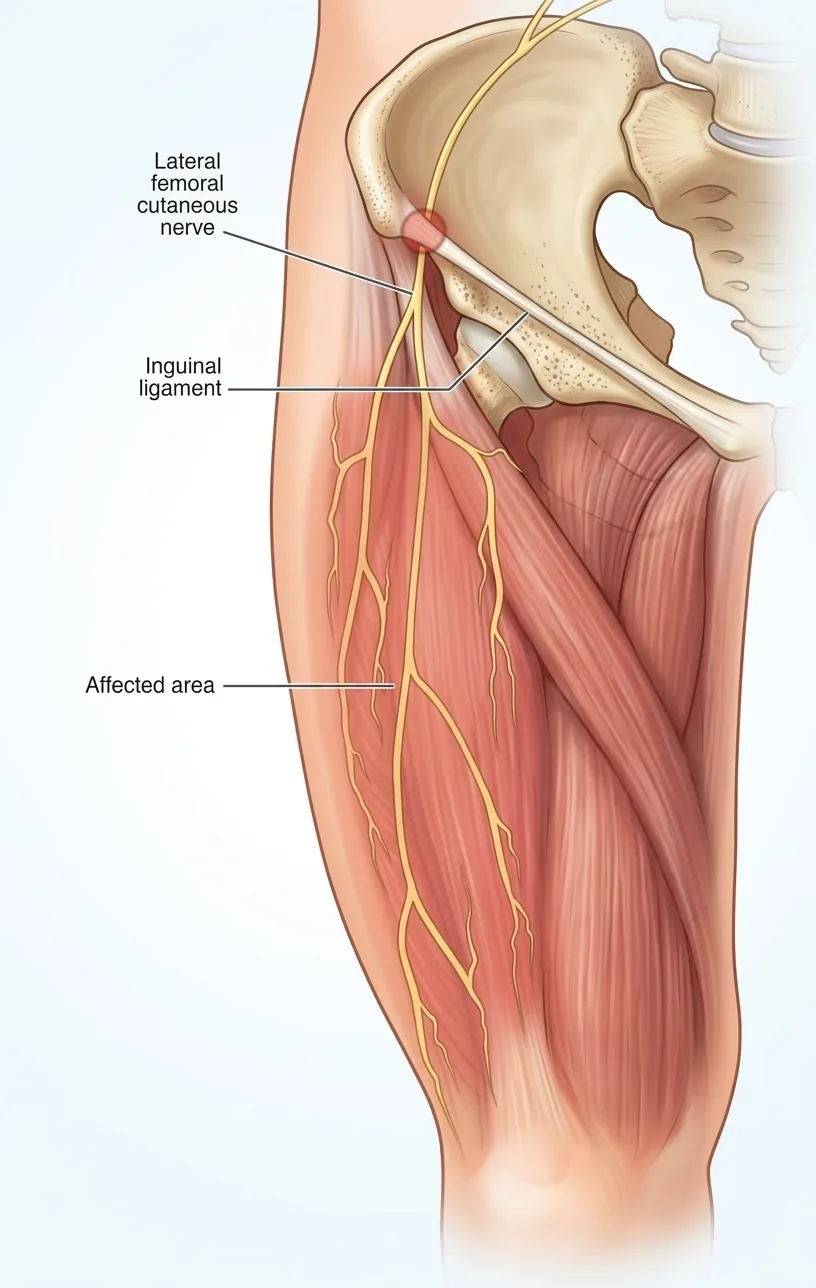
Meralgia paresthetica. The lateral femoral cutaneous nerve, which runs along the outside of the thigh, is compressed near the front of the hip and causes burning and numbness on the outer thigh. A 2024 randomized double-blind trial in Pain Physician by Shi et al. compared ultrasound-guided 5% dextrose hydrodissection to corticosteroid hydrodissection for meralgia paresthetica and found the dextrose group had greater improvement in pain and quality of life at 4 and 6 months, along with no reported adverse effects compared to six adverse events in the steroid group.
Vagus and cervical autonomic nerves. The vagus nerve runs through the side of the neck and regulates autonomic function (heart rate, digestion, vocal-cord control). Compression or chronic irritation of the vagus and surrounding cervical autonomic structures has been linked to chronic multisite pain and autonomic dysfunction in case-report literature. Learn more about vagus nerve hydrodissection and who it helps.
Post-surgical nerve adhesions. After surgery, scar tissue can form around nerves, creating new entrapments. Hydrodissection can free these adhesions without additional surgery.
Other peripheral nerve entrapments. The peroneal nerve at the knee, the sural nerve at the ankle, the saphenous nerve, sciatic nerve branches, branches of the cervical plexus, the superior cluneal nerves where they cross the top of the pelvis, and others can develop entrapments that respond to hydrodissection.
When Is Nerve Hydrodissection Not the Right Fit?
Nerve hydrodissection is not the right fit for patients with generalized peripheral neuropathy without a focal entrapment, or for patients whose symptoms originate from a spinal nerve root rather than a peripheral nerve compression.
Generalized peripheral neuropathy (the kind of widespread nerve damage seen in long-standing diabetes) typically does not respond as well to hydrodissection because the problem is diffuse rather than localized to a specific compression point. There is emerging evidence for PRP-based perineural treatment in selected diabetic-nerve cases, but the strongest candidates for hydrodissection are patients with a clearly identifiable single nerve compressed at a specific location. Symptoms originating from a spinal nerve root rather than a peripheral nerve compression also call for a different approach (typically spine-focused interventions or imaging-guided spinal injections rather than peripheral hydrodissection).
What Injectates Are Used in Nerve Hydrodissection?
Nerve hydrodissection can be performed with several injectates: 5% dextrose in water (D5W), platelet-rich plasma (PRP), platelet lysate, protein concentrate (A2M), bone marrow concentrate, and microfragmented adipose tissue. The choice depends on the diagnosis, the chronicity of the entrapment, and the imaging findings.

The published evidence is dominated by D5W, the most-studied injectate, with randomized trials supporting its safety and efficacy across carpal tunnel syndrome (Wu et al. 2017), occipital neuralgia (Lam et al. 2024), meralgia paresthetica (Shi et al. 2024), and a range of other peripheral nerve entrapments (Buntragulpoontawee et al. 2021). D5W works, it is forgiving, and the safety profile is excellent.
At Regenerative Performance, the primary injectate for nerve hydrodissection is platelet-rich plasma combined with protein concentrate (also called A2M, alpha-2-macroglobulin). PRP delivers concentrated platelet-derived growth factors directly to the nerve surface, and the PRP randomized trials at the median nerve indicate that a single PRP injection can produce meaningful 6-month and 1-year improvement in carpal tunnel cases. Protein concentrate is layered alongside PRP because it carries proteins, additional growth factors, and signaling peptides (some at higher concentrations than PRP alone) that assist the tissue-healing response. In our clinical experience, fewer treatment sessions are typically required when PRP combined with protein concentrate is the primary injectate compared with D5W standalone.
We do not treat this as PRP versus D5W. When we perform nerve hydrodissection with PRP and protein concentrate, we typically add 5% dextrose to the injectate. Patients receive both the orthobiologic effect of PRP and the established analgesic effect of D5W in a single procedure.
For selected cases, we use other autologous orthobiologics depending on what the diagnosis warrants:
- Platelet lysate when a more concentrated, growth-factor-released form of platelet content is preferred, or when a patient's blood profile makes standard PRP less practical
- Bone marrow concentrate (autologous stem cells from the iliac crest) when the entrapment is severe, longstanding, or accompanied by significant nerve structural change on ultrasound
- Microfragmented or nano-fragmented adipose tissue (autologous stem cells from a small fat harvest) when bone marrow is not the right fit and a stem-cell-based approach is indicated
Selection is based on the diagnosis, the chronicity of the entrapment, the patient's overall health, and the imaging findings. The decision is made during the evaluation, not by template.
A note on the published evidence: most randomized trials of nerve hydrodissection use D5W standalone because D5W is inexpensive, easy to standardize across study sites, and free of the biologic variability that complicates trial design. The PRP randomized-trial evidence is concentrated at the median nerve. Across the rest of the body, the strongest published evidence is for D5W. Our protocol is built on the existing PRP evidence at the median nerve, the established safety and analgesic effect of D5W at multiple sites, and several years of in-clinic experience treating focal nerve entrapments across the upper and lower extremity, the head, and the autonomic nerves of the neck.
What Makes Nerve Hydrodissection Different from a Nerve Block?
Nerve hydrodissection differs from a nerve block in that hydrodissection uses fluid pressure to physically separate a trapped nerve from the tissue compressing it, while a nerve block injects anesthetic near a nerve to temporarily numb pain signals. A nerve block numbs; hydrodissection frees.
A nerve block injects anesthetic (and sometimes steroid) near a nerve to temporarily interrupt pain signals. The goal is symptom relief that lasts hours to weeks. The nerve itself is not moved, freed, or healed. When the medication wears off, if the structural compression is still there, the pain returns.
Nerve hydrodissection physically changes the anatomy around the nerve. The fluid creates a plane of separation between the nerve and the tissue compressing it. When orthobiologics like PRP are used, the growth factors continue working on the nerve and surrounding tissue for days to weeks after the procedure. The goal is to restore normal nerve function, not to temporarily suppress the pain signal.
The ultrasound-guided technical standard for nerve hydrodissection is also more demanding than a typical nerve block. A 2021 systematic review in Frontiers in Pharmacology by Buntragulpoontawee et al. evaluated the most commonly used injectates and concluded that real-time ultrasound guidance is what enables precise circumferential fluid placement around the nerve, an effect that is not achievable with landmark-based or palpation-guided techniques.
Why Do Some Nerve Hydrodissection Treatments Fail?
When a patient has had a nerve hydrodissection elsewhere and the procedure did not produce meaningful improvement, three factors are usually responsible.
Technique. Proper hydrodissection requires meticulous, slow needle work and complete circumferential spread of the injectate around the nerve. A point injection that places fluid near the nerve but does not lift the surrounding fascia off the nerve circumferentially is, mechanically, a slightly fancier nerve block. Achieving 360-degree spread takes time, multiple needle redirections, and often following the nerve along its course rather than treating a single point. This is the difference between a five-minute injection and a 20- to 45-minute procedure.
Injectate selection. What is in the syringe matters. PRP and PRP-based biologics deliver concentrated growth factors that the nerve and surrounding tissue absorb over the following days, providing both mechanical decompression and a sustained biological repair signal. D5W is the most-studied option and has a strong safety profile, but in clinical experience tends to require more sessions than PRP for comparable improvement at the same nerve. Steroid hydrodissection has an analgesic effect but carries documented adverse-event risk; the 2024 Pain Physician trial of D5W versus corticosteroid for meralgia paresthetica reported six adverse events in the steroid group versus none in the dextrose group.
Diagnostic accuracy. A perfectly executed hydrodissection of the wrong nerve, or of the right nerve at the wrong location, will not improve the patient. Examples include treating thoracic outlet symptoms when the actual driver is cervical radiculopathy, or releasing the carpal tunnel when the median nerve is also compressed at the pronator teres in the forearm. The diagnosis has to be right before the technique can matter. This is why the 2-hour evaluation, hands-on exam, and diagnostic ultrasound come before any injection at Regenerative Performance.
If you have been told nerve hydrodissection did not work for you, or you are weighing it as an option for the first time, the most useful next step is an evaluation that re-examines the diagnosis from the ground up.
Schedule a comprehensive 2-hour evaluation for your nerve pain at Regenerative Performance.
Outcome Snapshot
Among the 109 cases with completed safety follow-up in our registry, zero severe treatment-related adverse events have been recorded, in registry data collected over more than 5 years. More than 95% of wrist and hand patients followed past 12 months in our outcome registry report significant pain relief; at 3 months, 89% report significant pain relief. Foot and toe cases (many of which involve nerve components) show more than 95% of patients reporting significant pain relief at 6 months and 18 months.
Note on registry data. Registry data from our single practice, powered by DataBiologics, is not a randomized clinical trial. Individual results may vary.
What to Expect at Regenerative Performance for Nerve Hydrodissection
The evaluation process is where hydrodissection outcomes are made or lost. Injecting a nerve without a thorough diagnostic workup is how treatments fail.
Comprehensive 2-Hour Evaluation
Every new patient at Regenerative Performance receives a full evaluation that begins with a detailed history and a hands-on physical exam. The physical exam is the primary diagnostic tool, not imaging. Specific provocative tests reproduce your symptoms and identify which nerve is involved and where the entrapment is occurring.
Individualized Treatment Plan
After the physical exam narrows the diagnosis, diagnostic ultrasound confirms and supports the findings. The ultrasound can visualize nerve swelling, fascial thickening, and the exact point of compression. The treatment plan that comes out of the evaluation specifies which nerves need treatment and what injectate will be used (typically PRP combined with protein concentrate, sometimes layered with 5% dextrose). Treatment is taken one injection at a time; whether a second session is appropriate is decided at the follow-up evaluation based on response, not predicted in advance.
Ultrasound-Guided Nerve Hydrodissection
The procedure is performed in the office, typically taking 20 to 45 minutes depending on the number of nerves treated. Under real-time ultrasound guidance, the needle is advanced to the entrapment site and the injectate is delivered with 360-degree spread around the nerve.
Recovery and Follow-Up
Most patients drive themselves home and return to light activities within 1 to 2 days. Improvement typically begins to register at 2 to 3 months as the inflammation around the nerve resolves and the growth factors support tissue repair. Continued improvement builds through 3 to 6 months. A follow-up evaluation re-examines the nerve on ultrasound and assesses whether a second session would benefit the case.
Who Is a Good Candidate for Nerve Hydrodissection?
The right candidate for nerve hydrodissection typically fits most of these criteria.
- Diagnosed with or suspected of having a specific peripheral nerve entrapment (carpal tunnel, cubital tunnel, tarsal tunnel, occipital neuralgia, meralgia paresthetica, or another focal nerve compression)
- Experiencing symptoms for 3 or more months, including numbness, tingling, burning, weakness, or pain along a nerve distribution
- Failed conservative care including medications, physical therapy, bracing, or nerve blocks
- Steroid injections or nerve blocks that helped temporarily but wore off
- Looking for a non-surgical option before considering surgical nerve release
- Interested in a structure-specific treatment that targets the exact site of compression
- Prepared for an out-of-pocket investment; nerve hydrodissection with biologics is not typically covered by insurance
Nerve hydrodissection is generally not the right fit for patients with generalized peripheral neuropathy without a focal entrapment, or for patients whose symptoms are coming from a spinal nerve root issue rather than a peripheral nerve compression. During your first visit, the provider confirms whether hydrodissection or another approach is appropriate and discusses other options if it is not the right fit.
We limit how many new regenerative patients we accept each month to maintain the quality of our diagnostic evaluations and procedures.
Call 480-508-4226 Work With Us
Frequently Asked Questions About Nerve Hydrodissection
Is nerve hydrodissection painful?
Nerve hydrodissection causes only minimal discomfort during the procedure for most patients. The ultrasound-guided approach allows precise needle placement, which reduces unnecessary tissue disruption, and the fine-gauge needles used are well-tolerated.
How long do nerve hydrodissection results last?
When nerve hydrodissection successfully releases a trapped nerve, many patients experience lasting improvement. Most patients begin to notice changes within 2 to 3 months, with continued improvement over 3 to 6 months and meaningful benefit often persisting at a year or longer in our clinical experience. When PRP or other orthobiologics are used, growth factors continue working on the nerve and surrounding tissue for weeks after the procedure. Some patients need a second session to achieve full release, particularly when the entrapment is longstanding.
How effective is nerve hydrodissection?
Nerve hydrodissection has the strongest published evidence at the median nerve, where multiple randomized controlled trials (Wu 2017, Chen 2021) suggest meaningful improvement at 6 months and one year for carpal tunnel syndrome. Effectiveness depends heavily on diagnostic accuracy, technique quality, and injectate selection.
In our outcome registry, more than 95% of wrist and hand patients followed past 12 months report significant pain relief.
Is nerve hydrodissection covered by insurance?
No, nerve hydrodissection is not typically covered by insurance, particularly when PRP or other biologic solutions are used. This applies regardless of which state you live in. The procedure is a cash-pay investment.
How does nerve hydrodissection compare to surgical nerve release?
Surgical nerve release and hydrodissection aim to accomplish the same fundamental goal of freeing a trapped nerve. Surgery does this by cutting the tissue compressing the nerve. Hydrodissection does it by using fluid pressure to separate the nerve from the tissue without cutting anything. Surgery carries risks of infection, anesthesia complications, nerve damage, and scar tissue formation that can create new entrapments. Hydrodissection is performed in the office, requires no general anesthesia, and has minimal downtime.
Can nerve hydrodissection treat carpal tunnel without surgery?
Yes, nerve hydrodissection can treat carpal tunnel syndrome non-surgically by using fluid pressure to separate the median nerve from the transverse carpal ligament compressing it. The published research is strongest for the median nerve, and PRP-based hydrodissection has suggested meaningful improvement at one year in moderate-to-severe cases.
What injectate is best for nerve hydrodissection: PRP, dextrose, or steroid?
PRP delivers the most concentrated growth-factor effect and has the strongest randomized-trial evidence at the median nerve. 5% dextrose has the largest published evidence base across other body regions and a strong safety profile. Steroid injections have an analgesic effect but documented adverse-event risk in head-to-head trials with dextrose for meralgia paresthetica (see References). Regenerative Performance typically combines PRP with A2M protein concentrate layered with 5% dextrose, so patients receive both the orthobiologic effect and the established analgesic effect of D5W in one procedure.
Does nerve hydrodissection work for peripheral neuropathy from diabetes?
Nerve hydrodissection typically responds less well to generalized peripheral neuropathy from long-standing diabetes than to focal nerve entrapments. The problem in generalized neuropathy is diffuse rather than localized to a specific compression point, and hydrodissection is best suited to releasing focal mechanical compression. There is emerging evidence for PRP-based perineural treatment in selected diabetic-nerve cases, but it remains a less-established application than focal-entrapment hydrodissection.
Still have questions? The best way to get answers is a conversation. Call 480-508-4226.
Medical Disclaimer
Nerve hydrodissection with platelet-rich plasma or other autologous biologics is an off-label application of devices cleared to prepare platelet concentrates. It is not an FDA-approved treatment for nerve entrapment. All procedures at Regenerative Performance are performed under ultrasound guidance. Results vary by patient and condition. The information on this page is educational and does not constitute medical advice. We need to evaluate your specific situation before determining if nerve hydrodissection makes sense for you.
About Dr. Drew Timmermans

Dr. Drew Timmermans, ND, RMSK
Drew Timmermans, ND, RMSK, is the founder of Regenerative Performance and specializes in precision-guided orthobiologic injections for chronic musculoskeletal and nerve pain. His approach starts with a thorough 2-hour evaluation that includes a hands-on physical exam and diagnostic ultrasound to identify the specific structures causing pain.
He is one of a small number of providers performing advanced ultrasound-guided nerve hydrodissection with platelet-rich plasma and other autologous orthobiologics. Read Dr. Timmermans's full bio.
References
- Wu YT, Ho TY, Chou YC, Ke MJ, Li TY, Tsai CK, Chen LC. Six-month efficacy of platelet-rich plasma for carpal tunnel syndrome: A prospective randomized, single-blind controlled trial. Sci Rep. 2017;7:94. DOI: 10.1038/s41598-017-00224-6.
- Wu YT, Ho TY, Chou YC, Ke MJ, Li TY, Huang GS, Chen LC. Six-month efficacy of perineural dextrose for carpal tunnel syndrome: A prospective, randomized, double-blind, controlled trial. Mayo Clin Proc. 2017;92(8):1179-1189. DOI: 10.1016/j.mayocp.2017.05.025.
- Chen SR, Shen YP, Ho TY, Li TY, Su YC, Chou YC, Chen LC, Wu YT. One-year efficacy of platelet-rich plasma for moderate-to-severe carpal tunnel syndrome: A prospective, randomized, double-blind, controlled trial. Arch Phys Med Rehabil. 2021;102(5):951-958. DOI: 10.1016/j.apmr.2020.12.025.
- Shen YP, Li TY, Chou YC, Ho TY, Ke MJ, Chen LC, Wu YT. Comparison of perineural platelet-rich plasma and dextrose injections for moderate carpal tunnel syndrome: A prospective randomized, single-blind, head-to-head comparative trial. J Tissue Eng Regen Med. 2019;13(11):2009-2017. DOI: 10.1002/term.2950.
- Lam KHS, Hung CY, Wu TJ, Chen KH, Reeves KD, Mubarak HK. Novel ultrasound-guided hydrodissection with 5% dextrose for the treatment of occipital neuralgia targeting the greater occipital nerve. Diagnostics (Basel). 2024;14(13):1380. DOI: 10.3390/diagnostics14131380.
- Shi C, Jia Z, Xu H, et al. A randomized double-blind trial of 5% dextrose versus corticosteroid hydrodissection for meralgia paresthetica. Pain Physician. 2024;27:E835-E842. DOI: 10.36076/ppj.2024.7.e835.
- Buntragulpoontawee M, Chang KV, Vitoonpong T, Pornjaksawan S, Kitisak K, Saokaew S, Kanchanasurakit S. The effectiveness and safety of commonly used injectates for ultrasound-guided hydrodissection treatment of peripheral nerve entrapment syndromes: A systematic review. Front Pharmacol. 2021;11:621150. DOI: 10.3389/fphar.2020.621150.
NOTE: This article provides general information to help the reader better understand regenerative medicine, nerve and musculoskeletal conditions, naturopathic approaches to pain, and related subjects. All content provided in this article, website, or any linked materials, including text, graphics, images, research, and outcomes, are not intended, and should not be used, as a substitute for direct medical advice, diagnosis, or treatment. Please always consult with a professional and licensed healthcare provider to discuss if any treatment is right for you.
Registry data from our single practice, powered by DataBiologics, is not a randomized clinical trial. Individual results may vary.