Alternatives to Knee Replacement: What the Evidence Shows
Short Answer
- If you have been told you need a knee replacement for bone-on-bone osteoarthritis, you have real non-surgical alternatives that an orthopedic surgeon may not have discussed in depth.
- The strongest non-surgical options use your body's own biology, in particular platelet-rich plasma (PRP) and bone marrow concentrate, delivered with image guidance to the structures causing your pain.
- Published research and our own knee patient outcomes show meaningful improvements in pain and function within 4 to 12 weeks, with results that often last well beyond the first year.
For adults in Scottsdale, Paradise Valley, and the greater Phoenix area who have been told they are "bone on bone," the conventional path runs the same way: physical therapy, anti-inflammatories, a series of cortisone shots, maybe a round of hyaluronic acid injections, and then a surgical consult. Physical therapy can genuinely help some people; anti-inflammatories and cortisone shots calm inflammation and pain without changing the joint; hyaluronic acid can ease symptoms for a while. What this sequence rarely does is treat the structure of the joint itself. By the time a surgical date is on the calendar, most patients have never had a real conversation about regenerative options, treatments that deliver your own platelets or bone marrow cells to the damaged tissue and that often improve function in the people who arrive after that conventional sequence has run out.
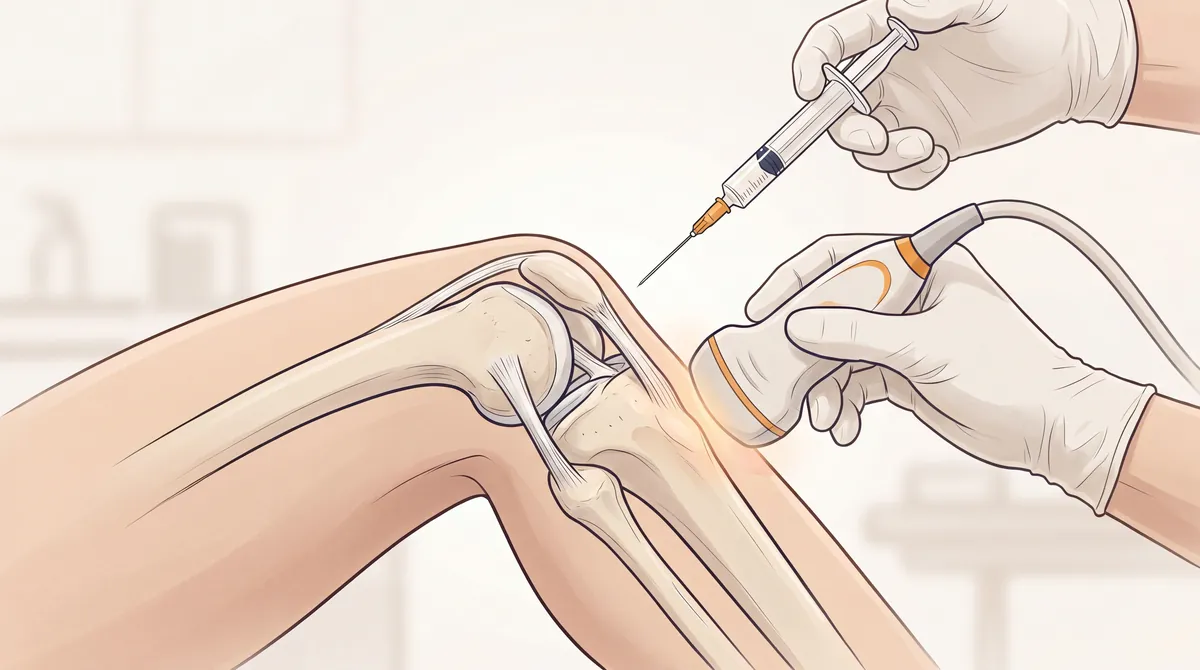
Non-surgical alternatives to knee replacement use image-guided orthobiologic injections (platelet-rich plasma, bone marrow concentrate, and related regenerative options), delivered with ultrasound for soft-tissue and joint targets and with fluoroscopic guidance for injections into the subchondral bone, to support the healing capacity of the joint tissues rather than removing and replacing them. At Regenerative Performance in Gilbert, AZ, we serve Scottsdale-area patients with chronic knee pain who want to know whether their joint is still a candidate for a biological repair approach before they commit to surgery. These treatments do not work for every knee, and we screen carefully to determine candidacy.
If you have already tried physical therapy, anti-inflammatories, or cortisone injections without lasting relief, the next step is a comprehensive evaluation that figures out what is actually generating the pain. Call us at 480-508-4226 to schedule a 2-hour evaluation for your knee.
Many of our knee osteoarthritis patients travel from Scottsdale, Paradise Valley, and across the greater Phoenix area after exhausting conventional care. Several have reported sustained improvement after properly dosed, image-guided orthobiologic injections combined with a structured rehabilitation plan, including patients who arrived at our clinic with a surgical date already on the calendar.
This page is especially useful if you have been told you are "bone on bone," your cortisone or gel injections have stopped working, and you live in or near Scottsdale, AZ.
What Does "Bone on Bone" Actually Mean for Your Knee?
"Bone on bone" is the phrase orthopedic clinics use when an x-ray shows the cartilage layer between the thigh bone and the shin bone has worn thin enough that the two bones appear to touch in the image. It usually means the knee has reached Kellgren-Lawrence grade 3 or grade 4 osteoarthritis, a staging system based on the x-ray appearance of joint-space narrowing, bone spurs, and bone-surface changes.
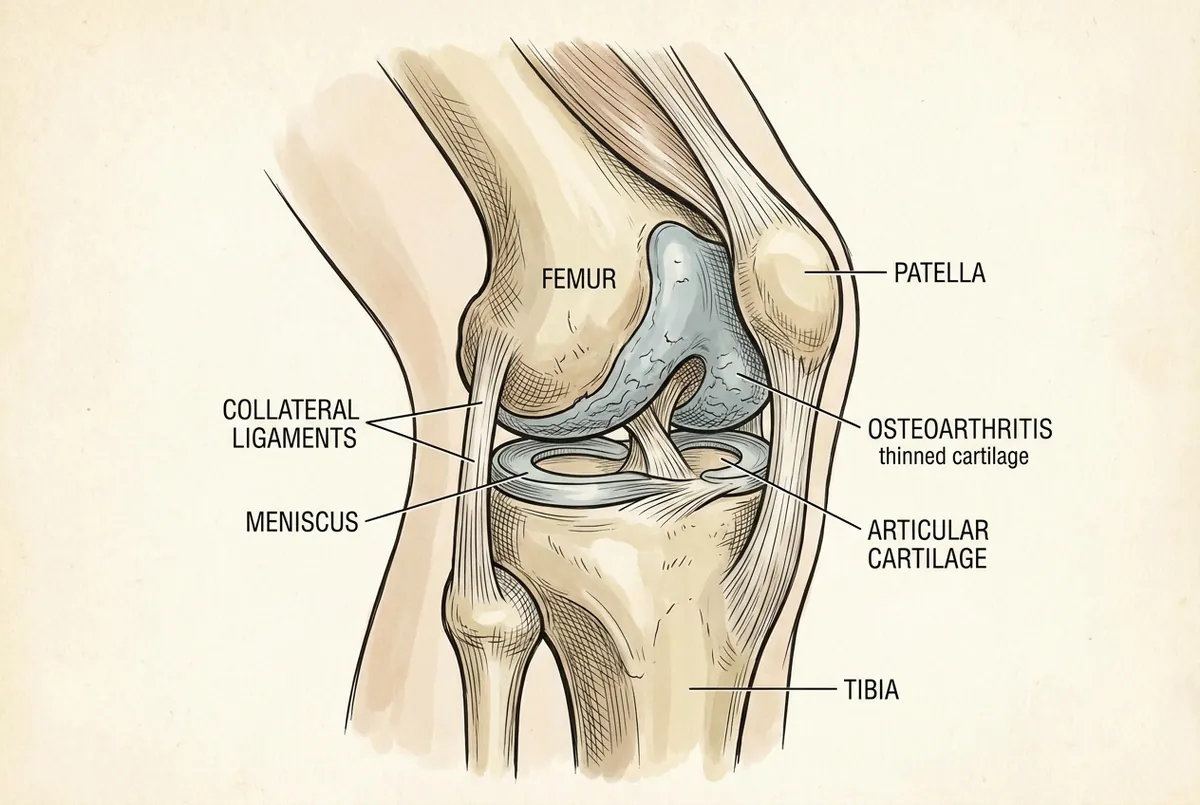
The phrase is technically accurate but psychologically loaded. Most patients hear "bone on bone" and assume the only option left is to remove the joint and put in a metal-and-plastic replacement. That assumption skips two important points. First, the worn cartilage itself is not what hurts. Articular cartilage has no blood supply and no nerve endings, so the cartilage layer cannot generate pain on its own. As it thins, the load it used to cushion transfers to the bone underneath, and that subchondral bone responds with microfractures, swelling inside the bone (bone marrow edema), and the pain that comes with them. The subchondral bone is one of the main pain generators in an arthritic knee. The ligaments around the joint, the meniscus, the joint lining, the fat pad behind the kneecap, and the small nerves that supply the joint can each be primary contributors as well. Second, pain severity does not always match imaging severity, which is why some patients with severe-looking x-rays have manageable pain, and others with mild-looking x-rays struggle to walk.
The clinical implication is that "bone on bone" by itself does not tell you what is generating your pain. A careful evaluation, ideally with hands-on examination and diagnostic ultrasound, can usually identify which structures are most responsible. That is the question that determines whether a regenerative approach can help your knee specifically, or whether replacement really is the most reasonable next step.
What Are the 4 Categories of Non-Surgical Alternatives to Knee Replacement?
The non-surgical options for knee osteoarthritis fall into four evidence-tiered categories. We rank them here by the strength of the published evidence and by how directly each option addresses the underlying tissue rather than only the symptom of pain.
1. Orthobiologic injections (PRP and bone marrow concentrate)
Orthobiologic injections use a concentrated preparation of your own platelets or bone marrow cells, delivered with image guidance, ultrasound for the joint and soft tissue and fluoroscopy for the subchondral bone, to the specific structures of the knee that are generating pain. They are the strongest non-surgical category in the published evidence for delaying or avoiding total knee replacement, and they are RP's primary recommendation when candidacy is appropriate.
A 2024 review that pooled the best knee studies found that PRP gave more people meaningful, lasting pain relief than hyaluronic acid or other injections (Oeding et al., Am J Sports Med, 2024).
For bone marrow concentrate, the strongest long-term evidence comes from two 15-year randomized studies of subchondral injection, where the bone marrow stem cells are placed into the bone itself rather than only into the joint (Hernigou et al., Int Orthop, 2021a; 2021b). We cover that evidence, and what it means for an advanced "bone on bone" knee, in the section on subchondral bone marrow concentrate below.
2. Hyaluronic acid (visco-supplementation)
Hyaluronic acid injections (sometimes called "gel shots") add a viscous fluid to the joint to lubricate it and dampen the inflammatory response. They produce real but modest short-term symptom relief for some patients, and they remain a reasonable option for patients who are not candidates for orthobiologic injections.
When PRP and hyaluronic acid were compared head to head over five years, both helped, but PRP patients went noticeably longer before they needed another round of treatment (Di Martino et al., Am J Sports Med, 2019). The honest read is that hyaluronic acid works for some patients, but properly dosed PRP gives you a longer interval before the next injection is needed.
A separate randomized trial comparing the two found that PRP also outperformed hyaluronic acid on pain and stiffness from three to twelve months (Bansal et al., Sci Rep, 2021).
3. Cortisone (corticosteroid) injections
Cortisone has a defined role in knee osteoarthritis for acute flares and short-term symptom control, but it is the one option on this list that we generally recommend against for repeated long-term use. The reason is structural. A 2-year double-blind randomized clinical trial of patients with symptomatic knee osteoarthritis found that intra-articular triamcinolone (cortisone) injections every 12 weeks produced significantly greater cartilage volume loss on MRI compared to saline placebo, with no significant difference in knee pain between the two groups (McAlindon et al., JAMA, 2017).
Head-to-head against PRP, the gap shows up over time. In a randomized trial that followed patients with moderate knee osteoarthritis for a year, a single cortisone injection and a single PRP injection relieved knee pain about equally for the first month, but by three to four months PRP had moved meaningfully ahead and held that lead through the full year, while the cortisone benefit faded back toward where it started (Elksniņš-Finogejevs et al., J Orthop Surg Res, 2020). For a knee that is already short on cartilage, repeated cortisone works against the structure of the joint without delivering a lasting pain advantage. In our practice we almost never use cortisone for an osteoarthritic knee; we reserve it for the rare flare where it is genuinely the right call, and we do not recommend a repeated series.
4. Conservative care (physical therapy, weight loss, bracing)
Conservative care is the foundation that should support every other treatment on this list. Strong-evidence clinical guidelines (AAOS and OARSI) recommend supervised exercise programs and weight loss for symptomatic knee osteoarthritis because both have measurable effects on pain and function. A 5 to 10 percent reduction in body weight, when sustainable, reduces the load through the knee with every step. A focused strengthening program for the quadriceps, hip stabilizers, and gluteal muscles improves how the knee tracks under load.
Bracing has a more limited role. An unloader brace can help selected patients with isolated single-compartment disease, but it does not change the underlying tissue. Conservative care belongs alongside any regenerative treatment plan; it is rarely sufficient on its own for advanced disease, but its absence is a common reason that other treatments underperform.
Why Orthobiologic Injections Lead the Alternatives List for Knee Osteoarthritis
Orthobiologic injections are at the top of the evidence ranking because they are the only category that delivers material to the damaged tissue with the intent of supporting biological repair, rather than only relieving symptoms or replacing structure mechanically. Two factors determine whether they work for a specific knee: the accuracy of the diagnosis, and the dose and quality of the orthobiologic preparation delivered.
Key Facts About Orthobiologic Treatment for Knee Osteoarthritis
Here is what you need to know about orthobiologic injection treatment for knee osteoarthritis before deciding whether it is worth exploring.
- What it is: Image-guided injection of your own concentrated platelets (PRP) or bone marrow cells (BMC) into the specific structures of the knee that are generating pain, using ultrasound for the joint and soft tissue and fluoroscopy for the subchondral bone.
- Who it helps: Adults with chronic knee osteoarthritis (Kellgren-Lawrence grades 2 to 4) whose pain is originating from the knee joint, supporting ligaments, meniscus, or joint lining, and has not improved with physical therapy, anti-inflammatories, or cortisone injections.
- How it works: A concentrated biological preparation drawn from your own body is placed under image guidance (ultrasound for the joint and soft tissue, fluoroscopy for the subchondral bone) into the structures identified during the diagnostic evaluation. The platelets or cells release signaling molecules that recruit repair activity and modulate inflammation inside the joint.
- Goal of treatment: To support the joint's own healing capacity, reduce pain, and improve function, rather than masking the symptom or removing the tissue.
- Clinical outcomes: In our knee patients, nearly four out of five report significant pain relief by 18 months after treatment.
- Timeline: Most patients begin to notice changes within 4 weeks. Most of the improvement occurs over the first 3 months. Individual results may vary, and results from properly dosed orthobiologic injections can last more than two years.
- Typical treatments: We start with one orthobiologic session and track your individual response. A second session is considered 12 weeks later based on how you responded.
- Where: Regenerative Performance in Gilbert, AZ, serving Scottsdale, Paradise Valley, Tempe, Mesa, Chandler, and the greater Phoenix area.
- Next step: Call 480-508-4226 for a comprehensive 2-hour evaluation.
How PRP Works for Knee Osteoarthritis
Platelet-rich plasma is a preparation made from a sample of your own blood, spun to concentrate the platelets and the growth factors they release. When the concentrated platelets are injected into the joint and the supporting structures, they release signaling molecules that recruit repair cells and modulate the inflammatory response inside the joint. The biological effect is real but dose-dependent. Under-dosed PRP often gets written off as "PRP did not work," when the real problem was that the injection never delivered enough platelets to the tissue.
Two studies show why the dose matters. In a 2021 double-blind randomized trial of patients with moderate (predominantly Kellgren-Lawrence grade 3) knee osteoarthritis, a single PRP injection standardized to 10 billion platelets produced significantly greater clinical improvement at 12 months than a single hyaluronic acid injection. On follow-up MRI scans, far more of the PRP-treated knees showed no further cartilage loss than the hyaluronic-acid knees (Bansal et al., Sci Rep, 2021). A 2024 systematic review and meta-analysis focused on knee osteoarthritis then found that PRP injections delivering more than 10 billion platelets produced significantly greater functional improvement at 6 months compared with control treatments, while doses in the 5 to 10 billion range showed a more limited effect (Berrigan et al., Curr Rev Musculoskelet Med, 2024).
The bottom line on PRP for knee osteoarthritis: dose decides results. A properly dosed injection, more than 10 billion platelets, appears to work better than a low-dose one, especially for function, which is why how your PRP is prepared matters as much as getting PRP at all.
At Regenerative Performance, we have refined our PRP processing protocol so it consistently delivers more than 10 billion platelets into the knee, the dose the evidence points to as optimal, and we confirm the dose with an in-house check on every sample. The most common reason a regenerative treatment underperforms is a missed or incomplete diagnosis of which structures are actually driving the pain. Under-dosing is the next most common, and a consistent, confirmed protocol removes that second failure point.
Subchondral Bone Marrow Concentrate: Treating the Bone, Not Just the Joint
Bone marrow concentrate (BMC) is drawn from a sample of your own iliac crest bone marrow and processed to concentrate the nucleated cells, mesenchymal cells, and growth factors. It is a more involved procedure than PRP and is reserved for selected, often more advanced cases. What makes it powerful for a "bone on bone" knee is where it can be placed. BMC can be delivered into the joint itself (intra-articular, under ultrasound guidance), or it can be placed directly into the subchondral bone, the layer of bone just beneath the cartilage, under fluoroscopic (live x-ray) guidance. Because the subchondral bone is one of the main pain generators in advanced osteoarthritis, putting the biology exactly where the bone marrow lesions and microdamage live is a meaningfully different treatment than a joint injection alone.
The strongest long-term evidence for this approach comes from two 15-year randomized studies. In the first, each patient had one knee treated with a single subchondral BMC injection and the opposite knee replaced with a total knee replacement. By the 15-year mark, most of the bone-marrow-concentrate knees had still never needed a replacement, and the few that did were replaced years later than they otherwise would have been. On MRI, the bone marrow lesions in the treated bone shrank over the first two years (Hernigou et al., Int Orthop, 2021).
The second study compared the two delivery routes head to head, treating one knee with subchondral BMC and the other with an intra-articular BMC injection in the same patients. By 15 years, only about 20 percent of the subchondral knees had gone on to replacement, compared with about 70 percent of the intra-articular knees, evidence that placing the cells in the bone, not just the joint, is what postpones surgery (Hernigou et al., Int Orthop, 2021).
In our practice, subchondral bone marrow concentrate delivered under fluoroscopic guidance is the approach we have found most effective for advanced, bone-driven knee osteoarthritis, and it is built directly on this 15-year evidence. Earlier registry work on a specific BMC protocol also suggested a dose-response relationship, with higher nucleated cell counts associated with better pain outcomes; the authors call their finding preliminary and in need of randomized validation, but it points in the same direction as the PRP dose literature: the quality and placement of the biological preparation matter (Centeno et al., BMC Musculoskelet Disord, 2015).
Important note: In the United States, PRP and bone marrow concentrate for knee osteoarthritis are typically off-label uses of devices cleared to prepare platelet or cell concentrates, not FDA-approved treatments for knee osteoarthritis. The published evidence supports their use in appropriate candidates, but individual response varies and these procedures may not produce meaningful relief for every patient, nor are they a substitute for surgery when surgery is genuinely the right call.
Outcome Snapshot
Our outcomes registry tracks more than 340 cases across all treated body regions over the past five years. Within the knee cohort, patients report significant pain relief at the following rates after orthobiologic injection treatment:
Among patients treated specifically for osteoarthritis (knee, hip, shoulder), 75 percent report significant pain relief with an average pain reduction of 53 percent. Among the 109 cases with completed safety follow-up in our registry, zero severe treatment-related adverse events have been recorded, in registry data collected over more than 5 years.
Diagnosis and dose are what decide whether a regenerative approach works. Find out whether you can delay or avoid a knee replacement, by scheduling a comprehensive 2-hour evaluation at our Gilbert, AZ clinic (serving Scottsdale and the greater Phoenix area).
Who Is a Good Candidate for Non-Surgical Knee Treatment in Scottsdale, AZ?
A non-surgical regenerative approach is typically a good fit for adults with chronic knee osteoarthritis who have not responded to physical therapy, medications, or cortisone injections, and who want to address the structure of the joint before committing to a replacement. Our 2-hour evaluation is designed to confirm this for your specific situation.
Most patients who come to us with knee osteoarthritis share a similar profile. If you see yourself in the list below, an orthobiologic approach may be worth exploring.
- Location: Scottsdale, Paradise Valley, Tempe, Mesa, Chandler, Gilbert, or the greater Phoenix area
- Chronic knee pain for 3 months or longer, including pain that has been called "bone on bone"
- Failed conservative care including physical therapy, oral anti-inflammatories, weight loss, or bracing
- Cortisone injections that helped temporarily but no longer last, or that you have chosen to avoid
- Hyaluronic acid injections that have stopped delivering relief
- Looking for non-surgical options before committing to a knee replacement
- Want a structure-specific treatment that targets the exact joint, ligaments, and tissues generating your pain
- You are willing to invest in your health, as these are cash-pay procedures
A regenerative approach is generally not the right fit if your knee has reached severe mechanical instability, frank deformity, locking and giving way, or if you have medical conditions that prevent a safe injection procedure. In those cases, a knee replacement may genuinely be the most reasonable next step, and we will tell you that directly during the evaluation.
During your evaluation, we will assess whether PRP, bone marrow concentrate, or another regenerative protocol is the right approach for your knee, or whether you would be better served by a different treatment path.
If you are unsure whether orthobiologic injections like PRP or bone marrow concentrate are appropriate, or you are traveling from outside the Phoenix area, you can also call and ask about a brief 15 minute discovery call.
What to Expect at Our Scottsdale-Area Clinic for Knee Osteoarthritis
Regenerative Performance is located in Gilbert, AZ, roughly 20 minutes from most Scottsdale-area homes, and we treat patients from across the greater Phoenix area. Scottsdale patients can also visit our page on PRP therapy for Scottsdale residents. Every knee patient goes through the same four steps.
Comprehensive 2-Hour Evaluation
Every new patient starts with a detailed 2-hour evaluation that includes a thorough history, hands-on physical examination with specific tests for knee instability, meniscal injury, ligament laxity, and patellar tracking, plus diagnostic ultrasound when indicated. We test the knee joint, supporting ligaments, and surrounding tendons directly to determine whether they are the source of your pain, rather than relying solely on imaging.
We also screen with clinical neurodynamic tests to gauge how much of your pain is coming from the nerves in and around the knee. The primary purpose of this evaluation is to identify the specific tissues causing your pain. This step is crucial because proper diagnosis is the single most important factor in regenerative treatment success.
Individualized Treatment Plan
Based on the evaluation, we determine whether you are a candidate for PRP injection, bone marrow concentrate, or another regenerative approach. From there, we develop an orthobiologic plan specific to your case, including which structures will be treated, the expected timeline, and your role in recovery.
Because the first three months after an orthobiologic injection are the critical window where most healing occurs, we typically recommend supplements and peptides to support the healing process. Our goal is to give your body every advantage during that healing window.
Image-Guided Orthobiologic Injection
On your treatment day, we draw 120 to 300 mL of your blood, depending on how many structures we are treating. The preparation process typically takes one to one and a half hours because of how meticulous we are with processing. During this time, you relax in our IV lounge while we prepare your PRP using our standardized in-house protocol, which consistently delivers more than 10 billion platelets, the dose the evidence points to as optimal.
If your plan includes bone marrow concentrate, we also draw a small bone-marrow sample from the back of your pelvis and process it the same day before the injection. The knee joint, supporting ligaments, and any peri-articular structures identified during the physical exam are treated under ultrasound guidance, and when the plan calls for subchondral bone marrow concentrate, that injection is placed into the bone under fluoroscopic guidance. We treat each structure individually rather than relying on a single intra-articular injection.
Recovery and Follow-Up
After your injection, we recommend resting for the remainder of that day so your body can begin the healing process. Physical activity restrictions typically last 1 to 4 weeks, with a gradual return to full activity guided by your response. For most patients, we refer to a physical therapist who will design and adjust a rehabilitation plan specific to your treatment and goals.
In our clinic, most patients begin to notice changes within 4 weeks, with most of the improvement occurring over the first 3 months. Individual results may vary. We schedule follow-up assessments to track your progress using our outcome registry, giving both you and our team objective data on how your treatment is working.
Find out whether you can delay or avoid a knee replacement. Schedule a comprehensive 2-hour evaluation for your knee osteoarthritis at our Gilbert, AZ clinic.
Frequently Asked Questions About Alternatives to Knee Replacement
Can you live with bone-on-bone knees without surgery?
Many patients with bone-on-bone knee osteoarthritis manage their condition for years without a knee replacement, especially when they address conservative care, weight management, activity modification, and an evidence-based regenerative treatment plan. The pain in bone-on-bone osteoarthritis often comes from multiple structures around the joint rather than the worn cartilage surface itself, and treating those structures directly with image-guided orthobiologic injections can significantly reduce pain and restore function. Whether this is realistic for your specific knee depends on factors that a thorough evaluation can identify.
What is the most successful alternative to knee replacement?
By published evidence, image-guided orthobiologic injection (platelet-rich plasma or bone marrow concentrate) is the strongest non-surgical alternative for delaying or avoiding knee replacement in appropriate candidates. A 15-year within-patient randomized study found that a single subchondral bone marrow concentrate injection postponed or avoided knee replacement in most patients with bilateral medial-compartment osteoarthritis, with about 82 percent of treated knees never requiring a replacement during follow-up (Hernigou et al., Int Orthop, 2021). Properly dosed PRP also outperforms hyaluronic acid and other non-operative comparators in meta-analysis (Oeding et al., Am J Sports Med, 2024).
What is the regret rate for knee replacements?
Published studies typically report that 15 to 20 percent of patients are dissatisfied with their knee replacement outcome at one year or longer, with persistent pain, stiffness, or functional limitations as the most common reasons. The number is not negligible and is one of several reasons to consider all reasonable non-surgical options before committing to a replacement.
Are PRP injections better than cortisone for knee arthritis?
For long-term outcomes in knee osteoarthritis, the published evidence favors properly dosed PRP over repeated cortisone. A meta-analysis of randomized trials found PRP outperformed alternative non-operative treatments on the rate of achieving clinically meaningful pain improvement (Oeding et al., Am J Sports Med, 2024). On the cortisone side, a 2-year double-blind randomized trial found that repeated cortisone injections produced significantly greater cartilage volume loss than saline placebo, with no significant pain advantage (McAlindon et al., JAMA, 2017). Cortisone has a role for acute flares; it is not a long-term strategy for an osteoarthritic knee.
How long do PRP injections last for knee osteoarthritis?
Properly dosed PRP for knee osteoarthritis commonly provides relief that lasts one to two years or longer, and the benefit can often be extended with repeat treatment. In our outcome registry, knee patients who responded continue to report significant pain relief at the 18-month and 24-month marks. In a 5-year randomized trial of PRP versus hyaluronic acid, both treatments kept producing measurable improvement years after the initial series, with PRP patients going longer before they needed another round of treatment (Di Martino et al., Am J Sports Med, 2019). A separate study of early-stage knee osteoarthritis found that repeating the PRP cycle each year added further improvement at 18 months versus a single cycle (Gobbi et al., Knee Surg Sports Traumatol Arthrosc, 2015).
When should I consider knee replacement surgery instead of regenerative treatment?
Knee replacement is the more reasonable next step when the knee has reached the point of severe mechanical instability, frank deformity, locking or giving way, or when the patient has lifestyle goals that an orthobiologic approach realistically cannot support. We are not anti-surgery, and during the 2-hour evaluation we will tell you directly if your knee is past the window where a regenerative treatment can produce meaningful improvement.
What is the difference between PRP and bone marrow stem cells for knee arthritis?
PRP is a concentrated preparation of your own platelets and the growth factors they release, drawn from a blood sample. Bone marrow concentrate is a more involved preparation drawn from a sample of your own iliac crest bone marrow, processed to concentrate the nucleated cells, mesenchymal cells, and growth factors. PRP is the most-studied orthobiologic option for knee osteoarthritis and is appropriate for most candidates. Bone marrow concentrate is reserved for selected cases, often more advanced disease, where the additional cellular content is likely to add value. We determine which is the better fit during the 2-hour evaluation.
Am I a candidate for non-surgical treatment if my knee X-ray shows bone-on-bone?
A "bone on bone" reading on an x-ray does not automatically rule out a regenerative approach. Some patients with severe-looking imaging still have a knee that can respond well to orthobiologic treatment if the pain is being driven by structures the imaging does not show clearly, like the supporting ligaments or the joint lining. We use hands-on examination and diagnostic ultrasound to figure out where the pain is actually coming from before recommending a treatment.
How quickly will I see results from PRP for knee arthritis?
Most patients begin to notice changes within about 4 weeks, with the bulk of improvement over the first 3 months. By 6 months, 64 percent of our knee patients report significant pain relief, climbing to 79 percent by 18 months in our outcome registry. Individual results may vary, and a small number of patients require a second session at 12 weeks based on their response to the first.
Is PRP for knee osteoarthritis covered by insurance in Arizona?
Orthobiologic injections including PRP and bone marrow concentrate are generally not covered by insurance in Arizona, including Medicare. Regenerative Performance is a cash-pay clinic, which lets us spend the time a complex case actually requires and follow the evidence rather than the billing code. HSA and FSA funds can typically be applied toward services, and we provide superbills on request for self-submission. On a phone call or discovery call we can give you a fee range by body region and procedure type; your specific quote and treatment protocol come only after the clinician completes the new-patient evaluation and finalizes your working diagnosis and treatment plan.
Still have questions? The best way to get answers is a conversation. Call 480-508-4226.
About Dr. Drew Timmermans

Dr. Drew Timmermans, ND, RMSK
Dr. Drew Timmermans, ND, RMSK, is a naturopathic physician and registered musculoskeletal sonographer (RMSK) practicing at Regenerative Performance in Gilbert, AZ. He specializes in orthobiologic injections, including platelet-rich plasma, bone marrow concentrate, prolotherapy, perineural injection therapy, and nerve hydrodissection, using ultrasound and fluoroscopic guidance to treat the specific structures causing chronic pain rather than suppressing symptoms.
Dr. Timmermans has performed more than 10,000 orthobiologic injections since 2016, and contributes patient outcome data to the DataBiologics national registry to track responder rates and durability of treatment across thousands of cases. Read Dr. Timmermans's full bio.
References
- Oeding JF, Varady NH, Fearington FW, et al. Platelet-Rich Plasma Versus Alternative Injections for Osteoarthritis of the Knee: A Systematic Review and Statistical Fragility Index-Based Meta-analysis of Randomized Controlled Trials. Am J Sports Med. 2024;52(12):3147-3160. DOI: 10.1177/03635465231224463.
- Di Martino A, Di Matteo B, Papio T, et al. Platelet-Rich Plasma Versus Hyaluronic Acid Injections for the Treatment of Knee Osteoarthritis: Results at 5 Years of a Double-Blind, Randomized Controlled Trial. Am J Sports Med. 2019;47(2):347-354. DOI: 10.1177/0363546518814532.
- McAlindon TE, LaValley MP, Harvey WF, et al. Effect of Intra-articular Triamcinolone vs Saline on Knee Cartilage Volume and Pain in Patients With Knee Osteoarthritis: A Randomized Clinical Trial. JAMA. 2017;317(19):1967-1975. DOI: 10.1001/jama.2017.5283.
- Elksniņš-Finogejevs A, Vidal L, Peredistijs A. Intra-articular platelet-rich plasma vs corticosteroids in the treatment of moderate knee osteoarthritis: a single-center prospective randomized controlled study with a 1-year follow up. J Orthop Surg Res. 2020;15(1):257. DOI: 10.1186/s13018-020-01753-z.
- Bansal H, Leon J, Pont JL, et al. Platelet-rich plasma (PRP) in osteoarthritis (OA) knee: Correct dose critical for long term clinical efficacy. Sci Rep. 2021;11(1):3971. DOI: 10.1038/s41598-021-83025-2.
- Berrigan W, Tao F, Kopcow J, et al. The Effect of Platelet Dose on Outcomes after Platelet Rich Plasma Injections for Musculoskeletal Conditions: A Systematic Review and Meta-Analysis. Curr Rev Musculoskelet Med. 2024;17(11):523-533. DOI: 10.1007/s12178-024-09922-x.
- Hernigou P, Delambre J, Quiennec S, Poignard A. Human bone marrow mesenchymal stem cell injection in subchondral lesions of knee osteoarthritis: a prospective randomized study versus contralateral arthroplasty at a mean fifteen year follow-up. Int Orthop. 2021;45(2):365-373. DOI: 10.1007/s00264-020-04571-4.
- Hernigou P, Bouthors C, Bastard C, Flouzat Lachaniette CH, Rouard H, Dubory A. Subchondral bone or intra-articular injection of bone marrow concentrate mesenchymal stem cells in bilateral knee osteoarthritis: what better postpone knee arthroplasty at fifteen years? A randomized study. Int Orthop. 2021;45(2):391-399. DOI: 10.1007/s00264-020-04687-7.
- Centeno CJ, Al-Sayegh H, Bashir J, Goodyear S, Freeman MD. A dose response analysis of a specific bone marrow concentrate treatment protocol for knee osteoarthritis. BMC Musculoskelet Disord. 2015;16:258. DOI: 10.1186/s12891-015-0714-z.
- Gobbi A, Lad D, Karnatzikos G. The effects of repeated intra-articular PRP injections on clinical outcomes of early osteoarthritis of the knee. Knee Surg Sports Traumatol Arthrosc. 2015;23(8):2170-2177. DOI: 10.1007/s00167-014-2987-4.
NOTE: This article provides general information to help the reader better understand regenerative medicine, knee osteoarthritis, naturopathic approaches to pain, and related subjects. All content provided in this article, website, or any linked materials, including text, graphics, images, research, and outcomes, are not intended, and should not be used, as a substitute for direct medical advice, diagnosis, or treatment. Please always consult with a professional and licensed healthcare provider to discuss if any treatment is right for you.
Registry data from our single practice, powered by DataBiologics, is not a randomized clinical trial. Individual results may vary.