
Achilles Tendon Pain Treatment: What the Evidence Shows
Short Answer
- Most Achilles tendon pain comes from tendinopathy, which is a gradual degeneration of the tendon. Less often it comes from a partial-thickness tear, an insertional tendinopathy where the tendon meets the heel bone, or pain referred from another area.
- The evidence-based foundation of treatment is progressive loading rehab (eccentric or heavy-slow-resistance exercise) paired with an accurate diagnosis of which part of the tendon is involved.
- For pain that persists despite structured loading, carefully selected ultrasound-guided orthobiologic options may support repair in the right candidate, though individual results may vary and these are not a guaranteed fix.
Diagnosing the exact pain generator and concentrating a higher platelet dose are the two things we focus on to give an orthobiologic approach its best chance, and they are where our evaluation begins.
For active adults in Chandler, Gilbert, and Ahwatukee seeking non-surgical Achilles tendon treatment, the path before they arrive is usually the same: rest helped briefly, anti-inflammatories took the edge off without resolving anything, a heel lift and physical therapy gave partial relief, and now they are wondering whether an injection or surgery is the only thing left. The most important question is often the one that gets skipped: exactly which part of the tendon is actually driving the pain.
Achilles tendon pain treatment at Regenerative Performance starts with a thorough diagnostic workup, an in-depth history and a hands-on physical exam, followed by diagnostic musculoskeletal ultrasound when it is needed, which for Achilles pain it almost always is. We lead with the workup because the back of the heel can hurt for several different reasons, and imaging on its own only shows what might be involved, not what is actually causing the pain. The evidence-based foundation is progressive loading rehab, and for the right candidate whose pain persists, we offer ultrasound-guided platelet-rich plasma and other orthobiologic options to support repair. These treatments do not help every tendon, and we screen carefully before recommending any injection.
Find out which structure is actually driving your Achilles pain.
Many of our tendon patients travel from Chandler, Ahwatukee, and across the greater Phoenix area after a year or more of conventional care. Patients often arrive convinced their tendon is beyond help, when the real issue was that no one had identified the specific pain generator and treated it directly. Once the right structure is found and a proper loading and treatment plan is in place, many report a gradual return to walking, training, and standing through a full workday with less of the constant ache they had lived with.
Key Facts About Orthobiologic Treatment for Achilles Tendon Pain
Orthobiologic treatment for the Achilles is considered only after the diagnosis is clear and a structured loading program has had a fair trial.
- What it is: Ultrasound-guided injection of your own concentrated platelets (PRP) into the specific part of the Achilles tendon generating pain, used alongside, not instead of, a loading rehab program.
- Who it helps: Adults with chronic Achilles pain originating from midportion tendinosis, insertional tendinopathy, or a partial-thickness tendon tear that has not improved with a structured loading program, anti-inflammatories, or physical therapy.
- How it works: A concentrated preparation drawn from your own blood is placed under ultrasound guidance into the structure identified during the evaluation, where the platelets release signaling molecules that recruit repair activity in the degenerated tissue.
- Goal of treatment: Aims to support the tendon’s own repair and help ease pain over time, alongside the loading program, rather than masking the symptom.
- Clinical outcomes: Among tendinosis patients in our registry, more than 3 out of 4 report significant pain relief. Published randomized trials of single, low-dose injections for chronic midportion tendinopathy did not beat placebo, which is why diagnosis and dose matter. Individual results may vary.
- Timeline: Most patients begin to notice changes within 4 weeks, with most of the improvement occurring over the first 3 months. Individual results may vary.
- Typical treatments: We start with one orthobiologic session and track your individual response. A second session is considered 12 weeks later based on how you responded.
- Where: Regenerative Performance in Gilbert, AZ, serving Chandler, Ahwatukee, Tempe, Mesa, and the greater Phoenix area.
- Next step: Call 480-508-4226 for a comprehensive 2-hour evaluation.
What Does Achilles Tendon Pain Usually Mean?
Achilles tendon pain usually means tendinopathy, a degenerative change in the thick cord at the back of your heel and ankle that connects your calf muscles to your heel bone. The word patients hear most often is “tendinitis,” which implies simple inflammation, but the tissue change in long-standing Achilles pain is degeneration of the tendon fibers rather than active inflammation. That distinction matters, because it is one reason anti-inflammatory medication alone so often does not fix the problem.
Achilles pain does not all come from the same place, and the location of the problem changes the treatment. The pain may be coming from several different sources.
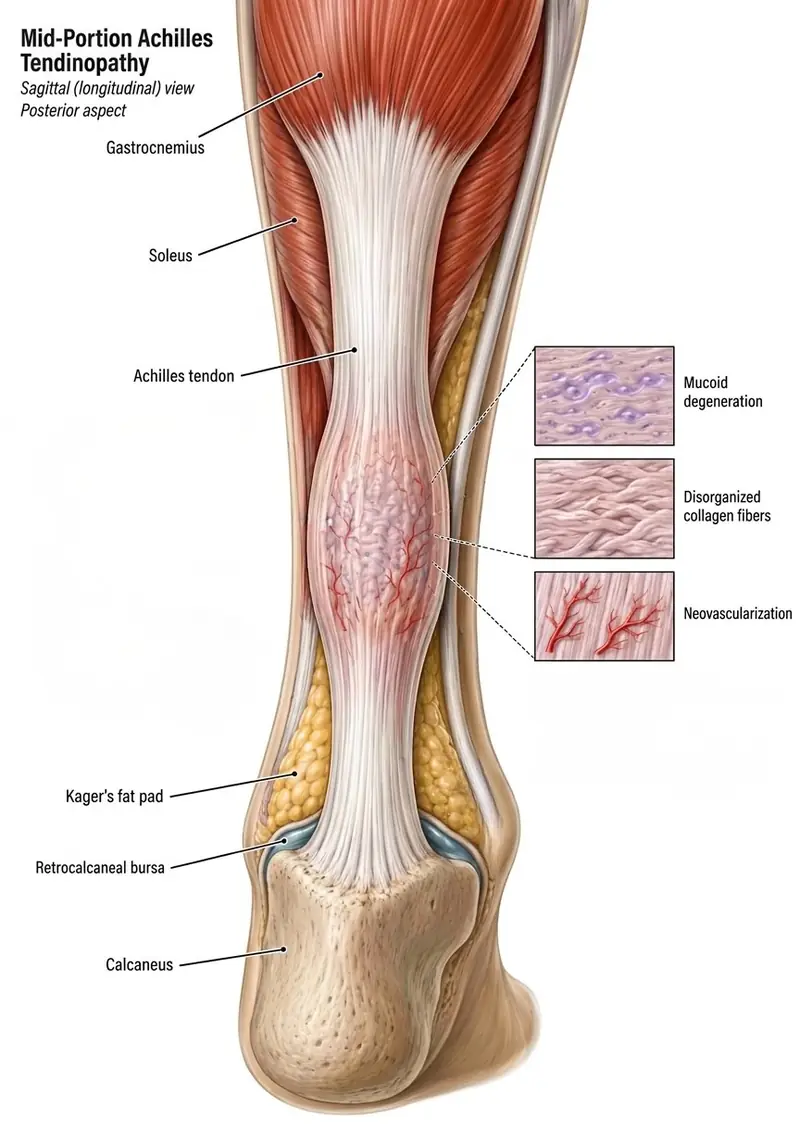
Midportion tendinopathy
This is the most common pattern, where the painful, sometimes thickened area sits a few centimeters above the heel bone in the main body of the tendon. Most of the published research on Achilles treatment focuses on this specific pattern.
Insertional tendinopathy
Here the pain sits right where the tendon attaches to the back of the heel bone. Insertional tendinopathy behaves differently from midportion tendinopathy and does not always respond to the same loading program, which is part of why an accurate diagnosis is worth the effort.
Partial-thickness tear
Some tendons have a partial-thickness tear, where a portion of the tendon fibers has actually pulled apart. This is a different problem from degeneration alone, and it is identified on imaging rather than guessed from symptoms.
Other sources of posterior heel pain
Pain at the back of the heel does not always come from the Achilles tendon itself. Several nearby structures can be the real driver, which is another reason a careful evaluation is the starting point rather than an assumption:
- Retrocalcaneal bursitis, inflammation of the small fluid-filled sac between the tendon and the heel bone
- Kager’s fat pad inflammation, irritation of the cushion of fat just in front of the tendon
- Flexor hallucis longus tendinopathy, involving a deeper tendon that runs alongside the Achilles
- Os trigonum syndrome, where a small extra bone at the back of the ankle gets pinched
- Sural neuropathy, irritation of a nerve that travels near the tendon
- Lumbosacral radiculitis, pain referred from an irritated nerve root in the lower back
Why the Right Diagnosis Comes First for Achilles Pain
The right diagnosis comes first because the back of the heel can hurt for several different reasons, and the correct treatment depends entirely on which structure is involved. Treating midportion degeneration, an insertional tendinopathy, a partial-thickness tear, or bursitis with the same generic plan is how good treatments end up falling short.
In our experience, the single most common reason a regenerative treatment underperforms is a missed or incomplete diagnosis of which structure is actually driving the pain. If a treatment is aimed at tissue that was never the pain generator, no amount of technique or preparation will make it work. This is why our evaluation leads with history and a hands-on physical exam, then uses diagnostic musculoskeletal ultrasound to confirm the finding.
Ultrasound is the primary imaging tool for tendon problems like the Achilles because it shows the soft tissue in real time, including the degenerated area, any partial-thickness tearing, and the blood-vessel changes that often accompany chronic tendon pain. As a registered musculoskeletal sonographer (RMSK), Dr. Timmermans performs this imaging directly, so the diagnosis and the treatment plan come from the same hands rather than a report passed between offices.

What Is the Most Effective Treatment for Achilles Tendon Pain?
The most effective and best-supported first-line treatment for Achilles tendon pain is progressive loading rehab, a structured strengthening program that gradually loads the tendon to drive it to remodel. This is the foundation, and for many patients it is enough on its own.
Loading rehab comes in two well-studied forms: eccentric exercise, where the calf slowly lowers under load, and heavy-slow-resistance training, where the tendon is loaded with heavier weight through a slower range. A controlled clinical trial of a 12-week high-loading program found that Achilles symptoms measured by the VISA-A score improved across all exercise groups, with tendon stiffness and cross-sectional area also increasing with the heaviest loading protocol (Radovanovic et al., Sports Medicine - Open, 2022). The mechanism is straightforward: tendons respond to load, and a graded program teaches the tissue to tolerate and rebuild under it.
The honest part of this picture is the timeline. Loading programs work over months, not weeks, and they require consistency to produce a durable result. Activity modification belongs alongside the program, dialing back the aggravating loads without going to complete rest, which tends to make tendons weaker. For a substantial number of patients, a well-run loading program plus an accurate diagnosis resolves the problem without any injection at all.
What Does the Research Actually Say About PRP for the Achilles?
The honest answer is that the strongest randomized trials of PRP for chronic midportion Achilles tendinopathy did not find it better than placebo when a single, often low-dose injection was used. This is the part of the conversation that many clinics skip, and we would rather you hear it from us directly.
The largest randomized trial to date, the PATH-2 study, enrolled 240 patients with chronic midportion Achilles tendinopathy and assigned them to a single intratendinous PRP injection or a sham injection, finding no meaningful improvement over the sham injection in tendon-related dysfunction at 6 months (Kearney et al., JAMA, 2021). A 2024 meta-analysis of six randomized trials encompassing 422 patients reached the same conclusion, finding no benefit of PRP over placebo on standard Achilles outcome measures, while specifically noting wide variability in how the PRP was prepared and dosed across trials and calling for standardized methods (Barreto et al., Clin Orthop Relat Res, 2024).
Taken at face value, that body of evidence says a generic, single PRP injection is not a reliable treatment for chronic midportion Achilles tendinopathy. We accept that. The more useful question is why those trials looked the way they did, and what that means for how a regenerative approach should actually be used.
Why “PRP Did Not Work in the Studies” Is Not the Whole Story
These studies answer a narrow question, which is whether a single, often low-dose PRP injection into a chronic midportion tendon beats a placebo shot. They do not test the way a careful regenerative practice actually works, and three differences matter.
The first is diagnosis. The most common reason a regenerative treatment underperforms is that the wrong structure was treated, or the true pain generator was never confirmed in the first place. Trials that enroll a broad “chronic midportion tendinopathy” label without confirming the specific pathology in each patient will dilute any real effect, because some of those tendons were never going to respond to that injection regardless of preparation.
The second is dose. Platelet concentration and total platelet dose are what separate a well-dosed PRP injection from a generic spin-and-inject, and the meta-analysis above flagged exactly this variability as a limitation. The PATH-2 preparation shows the problem: only about 9 mL of blood was drawn to make it, yielding a small, low-dose 3 mL of PRP. For comparison, a typical Achilles treatment at Regenerative Performance draws roughly 60 mL of blood to concentrate about 3 cc of far higher-dose PRP.
The dose-response evidence comes from other musculoskeletal conditions rather than the Achilles: a randomized trial in knee osteoarthritis found that a PRP preparation standardized to roughly 10 billion platelets produced durable one-year benefit (Bansal et al., Sci Rep, 2021), and a systematic review of musculoskeletal PRP found a dose-response relationship with better outcomes above a similar platelet threshold, while explicitly noting that the optimal dose for conditions outside the knee is less clear (Berrigan et al., Curr Rev Musculoskelet Med, 2024). Those findings are about dose mattering in general; they are not evidence that PRP resolves Achilles tendinopathy on its own, and the honest caveat about non-knee conditions is part of the point.
The third is image-guided delivery. Ultrasound guidance lets us place the needle in the exact structure we are treating, and many of the trials did not use it. In the PATH-2 study the injection was not performed under ultrasound, and only three of the six trials in the 2024 meta-analysis used ultrasound guidance at all. Whether guidance improves Achilles PRP outcomes specifically has not been settled, but we consider confirming needle placement a basic standard for putting the medicine where the imaging shows the problem. At Regenerative Performance, every orthobiologic injection is delivered under live ultrasound to the exact structure we identified.
This is the reasoning behind how we use orthobiologics: not as a blanket promise that PRP heals Achilles tendinopathy, but as a carefully selected option for the right pathology in the right patient, delivered to an accurately diagnosed target at a measured, higher platelet dose. That is a meaningfully different intervention from the single low-dose injection those studies tested.
Orthobiologic Options for Achilles Tendon Pain at Regenerative Performance
For an appropriately selected patient whose Achilles pain has persisted despite structured loading, the main orthobiologic option we consider is ultrasound-guided platelet-rich plasma (PRP). For milder cases centered on where the tendon attaches to the heel bone, prolotherapy can also be an option. Both are delivered under ultrasound guidance to the specific structure identified during the evaluation, and both are offered honestly as options that may support repair rather than as a certain cure.
PRP is the more studied of the two for tendon problems. Our PRP processing is standardized to consistently deliver a higher, measured platelet dose, and we test each sample in-house to confirm the platelet count. The pathology guides the decision. Chronic midportion tendinopathy that has failed a genuine loading program, insertional tendinopathy, and partial-thickness tendon tears are different problems, and we scope the conversation to your specific finding rather than a one-size-fits-all pitch. Where the imaging shows a partial-thickness tear, the consideration is different from degeneration alone, and our registry shows nearly 3 out of 4 patients with partial-thickness tears reporting significant pain relief.
The goal throughout is to support repair in the damaged tissue, not to mask the pain signal.
Please note: In the United States, PRP for Achilles tendinopathy is typically an off-label use of devices cleared to prepare platelet concentrates, not an FDA-approved treatment for Achilles tendinopathy. Published randomized trials of single PRP injections for chronic midportion tendinopathy have not shown benefit over placebo, and individual response varies. We present orthobiologic injection as a carefully selected option for appropriate candidates, not as a guaranteed solution.
Our Patient Outcome Registry
These outcomes come from our single-practice DataBiologics registry, a real-world observational dataset of patients treated at Regenerative Performance. Tendinosis (chronic tendon degeneration, the on-point diagnosis for most Achilles tendinopathy) is one of the strongest-performing diagnoses we track.
- Among tendinosis patients in our registry, more than 3 out of 4 report significant pain relief, with an average pain reduction of 62%.
- Among patients treated for a partial-thickness tendon tear specifically, nearly 3 out of 4 report significant pain relief.
- Among the 109 cases with completed safety follow-up in our registry, zero severe treatment-related adverse events have been recorded, in registry data collected over more than 5 years.
Diagnosis and dose are central to whether a regenerative approach can help your tendon.
Schedule a comprehensive 2-hour evaluation for your Achilles and lower-leg pain at our Gilbert, AZ clinic.
Our Position on Cortisone and Surgery for Achilles Pain
Patients often ask about cortisone and surgery, so here is where we stand on each. In short, we strongly recommend against corticosteroid injection into or around the Achilles, and surgery is the right call for only a minority of cases.
We do not use corticosteroid injection into or around the Achilles tendon, and we advise against it, because it can weaken the tendon and raise the risk of a rupture. Cortisone may quiet inflammation in the short term, but for a load-bearing tendon like the Achilles that trade is not worth it, and it does nothing for the underlying degeneration that is actually driving the pain. We mention this because patients sometimes ask why they were not simply offered a shot; the answer is that we are protecting the tendon.
Surgery is the more reasonable next step for some patients, including certain full-thickness tears and a portion of cases that have genuinely exhausted non-surgical care. We are not anti-surgery. The aim of a careful evaluation is to tell you honestly which category your tendon falls into, rather than steering every patient toward the same procedure.
Serving Chandler, Gilbert, and Ahwatukee.
Schedule a comprehensive 2-hour evaluation for your Achilles and lower-leg pain at our Gilbert, AZ clinic.
What to Expect at Our Chandler-Area Clinic for Achilles Tendon Pain
Regenerative Performance is located in Gilbert, AZ, a short drive from most Chandler-area homes, and we treat patients from across the greater Phoenix area. Every patient with Achilles tendon pain moves through the same four steps.

Comprehensive 2-Hour Evaluation
Every new patient starts with a detailed 2-hour evaluation that includes a thorough history, a hands-on physical examination, plus diagnostic ultrasound when indicated. We assess the Achilles tendon and surrounding structures directly to determine whether they are the source of your pain, rather than relying solely on outside imaging reports.
The primary purpose of this evaluation is to identify the specific structure causing your pain, because the right diagnosis is the single most important factor in whether a regenerative treatment works.
Individualized Treatment Plan
Based on the evaluation, we determine whether you are a candidate for a PRP injection or another regenerative approach, and how it should be paired with a loading program. From there, we develop an orthobiologic plan specific to your case, including which structure will be treated, the expected timeline, and your role in recovery.
During the first few months of recovery we may recommend supportive supplements and peptides as part of your plan.
Ultrasound-Guided PRP Injection
On your treatment day, we draw the amount of blood your case calls for, from roughly 60 mL for a single Achilles tendon up to a few hundred milliliters when several structures are treated in one visit. The preparation process typically takes one to one and a half hours because our in-house processing is standardized to deliver a measured platelet dose, and we verify the platelet count on every sample. During this time, you relax in our IV lounge.
The Achilles tendon and any related structures identified during the physical exam are treated under ultrasound guidance. We treat the specific pain-generating structure directly rather than injecting blindly into the general area.
Recovery and Follow-Up
After your injection, we recommend resting for the remainder of that day so your body can begin the healing process. Physical activity restrictions typically last 1 to 4 weeks, with a gradual return to full activity guided by your response. For most patients, we refer to a physical therapist who will design and adjust a loading and rehabilitation plan specific to your treatment and goals.
In our clinic, most patients begin to notice changes within 4 weeks, with most of the improvement occurring over the first 3 months. Individual results may vary.
We schedule follow-up assessments to track your progress using our outcome registry, giving both you and our team objective data on how your treatment is working.
Find out what is actually driving your Achilles pain. Schedule a comprehensive 2-hour evaluation for your Achilles and lower-leg pain at our Gilbert, AZ clinic.
Who Is a Good Candidate for Achilles Tendon Treatment in Chandler, AZ?
A regenerative approach is typically a good fit for adults with chronic Achilles tendon pain that has not responded to a structured loading program, anti-inflammatories, or physical therapy, and who want to address the tendon itself before considering surgery. Our 2-hour evaluation is designed to confirm this for your specific situation.
Most patients who come to us with Achilles pain share a similar profile. If you see yourself in the list below, an orthobiologic approach may be worth exploring.
- Location: Chandler, Ahwatukee, Tempe, Mesa, Gilbert, or the greater Phoenix area
- Chronic Achilles pain for 3 months or longer that has not settled with rest
- Worked through a loading or physical therapy program with only partial relief
- Active adult, runner, or weekend athlete who wants to get back to training
- Tried anti-inflammatories, a heel lift, or a walking boot without lasting change
- Looking for non-surgical options that target the tendon before considering surgery
- You are willing to invest in your health, as these are cash-pay procedures
A regenerative approach is generally not the right fit if the tendon has a full-thickness rupture that needs surgical attention, if you are seeking a single quick fix without doing the loading work, or if a medical condition makes a safe injection procedure unwise. In those cases we will tell you directly during the evaluation and point you toward the right path.
During your evaluation, we will assess whether PRP, prolotherapy, or another regenerative approach is appropriate for your specific tendon, or whether you would be better served by continued loading rehab or a surgical referral.
If you are unsure whether orthobiologic injections like PRP are appropriate, or you are traveling from outside the Phoenix area, you can also call and ask about a brief 15 minute discovery call.
Frequently Asked Questions About Achilles Tendon Pain
What is usually behind ongoing Achilles tendon pain?
Achilles tendon pain usually means tendinopathy, a degenerative change in the cord at the back of the heel and ankle, most often in the midportion of the tendon a few centimeters above the heel bone. Less commonly the pain comes from where the tendon attaches to the heel (insertional tendinopathy), a partial-thickness tear, or the small fluid-filled sac next to the tendon. Because these are different problems with different treatments, an accurate diagnosis is the starting point rather than an assumption from symptoms alone.
What is the difference between Achilles tendinitis and tendinosis?
Achilles tendinitis and tendinosis describe different stages of the same tendon problem. Tendinitis implies active inflammation, which is more typical of a recent flare, while tendinosis describes the degenerative fiber changes seen in long-standing Achilles pain. Most chronic Achilles pain is tendinosis, which is one reason anti-inflammatory medication alone often underperforms. Diagnostic ultrasound can show which pattern is present.
Does PRP work for Achilles tendinopathy?
PRP for chronic midportion Achilles tendinopathy has not outperformed placebo injection in the strongest randomized trials, which used single, often low-dose injections. The PATH-2 trial randomized 240 patients to a single PRP injection or sham and found no benefit at 6 months (Kearney et al., JAMA, 2021), and a 2024 meta-analysis of six randomized trials reached the same conclusion (Barreto et al., Clin Orthop Relat Res, 2024). Whether a regenerative approach helps an individual tendon depends on accurate diagnosis of the pain generator, the dose and quality of the preparation, the technique, and the specific pathology, which is why we present it as a carefully selected option rather than a guaranteed treatment.
What is the best first-line treatment for Achilles tendon pain?
Progressive loading rehab is the most effective and best-supported first-line treatment for Achilles tendon pain. A controlled clinical trial of a 12-week high-loading program found that Achilles symptoms improved across all exercise groups, with the VISA-A score increasing on average by 19.8 points, and tendon stiffness and cross-sectional area also increasing with the heaviest loading protocol (Radovanovic et al., Sports Medicine - Open, 2022). Loading works because tendons remodel in response to graded load, and for many patients a consistent program paired with an accurate diagnosis resolves the problem without any injection.
How long does Achilles tendinopathy take to heal?
Achilles tendinopathy typically improves over months rather than weeks, and a structured loading program usually needs to run for around three months or longer to produce durable change. Tendons change slowly, so consistency matters more than intensity. Where an orthobiologic injection is used, most patients begin to notice changes within 4 weeks, with most of the improvement occurring over the first 3 months. Individual results may vary.
Can I walk or run with Achilles tendon pain?
Most people with Achilles tendinopathy can keep walking and often keep running at a reduced level, because complete rest tends to make tendons weaker rather than better. The goal is to dial back the aggravating loads while keeping the tendon working through a graded program. Sudden sharp pain, a popping sensation, or marked weakness is a different situation that should be evaluated promptly, since it can signal a tear rather than tendinopathy.
Should cortisone shots be used for Achilles tendon pain?
We advise against corticosteroid injection into or around the Achilles because it can weaken the tendon and increase the risk of rupture. The Achilles is a heavily loaded tendon, and cortisone does nothing for the underlying degeneration that drives most chronic Achilles pain. It may quiet inflammation briefly, but for this tendon we do not consider that short-term relief worth the structural risk.
When should I consider an injection or surgery for Achilles pain?
An orthobiologic injection is typically considered when chronic Achilles pain has persisted despite a genuine loading program and the pathology is one that may respond, such as midportion tendinosis, insertional tendinopathy, or a partial-thickness tear confirmed on imaging. Surgery is reserved for a minority of cases, including certain full-thickness tears and patients who have truly exhausted non-surgical care. A thorough evaluation is what sorts your tendon into the right category rather than guessing.
How is Achilles tendon pain diagnosed?
Achilles tendon pain is diagnosed with a history, a hands-on physical examination, and diagnostic musculoskeletal ultrasound. Ultrasound is the primary imaging tool for the Achilles because it shows the soft tissue in real time, including the degenerated area, any partial-thickness tearing, and the blood-vessel changes that accompany chronic tendon pain. This combination helps identify the most likely source of the pain by correlating the imaging with the history and examination.
Is Achilles tendon treatment covered by insurance?
Orthobiologic injections including PRP are generally not covered by insurance. These injections are an off-label use of FDA-cleared devices used to prepare platelet concentrates and are not FDA-approved treatments for Achilles tendinopathy. Regenerative Performance operates as a cash-pay clinic, which means we can spend the time a complex tendon case actually requires and follow the evidence rather than the billing code. HSA and FSA funds can typically be applied toward services, and we discuss fees during your evaluation so we can match the right approach to your situation.
Who treats Achilles tendon pain in Chandler, AZ?
Achilles tendon pain in the Chandler area is treated by podiatrists, orthopedic and foot-and-ankle surgeons, physical therapists, and regenerative medicine clinics. At Regenerative Performance in Gilbert, Dr. Drew Timmermans, ND, RMSK, uses diagnostic ultrasound, correlated with the history and exam, to identify the most likely pain source before recommending treatment, and offers loading-rehab guidance plus ultrasound-guided orthobiologic options for candidates from Chandler, Ahwatukee, and across the greater Phoenix area.
Still have questions? The best way to get answers is a conversation. Call 480-508-4226.
About Dr. Drew Timmermans

Dr. Drew Timmermans, ND, RMSK
Dr. Drew Timmermans, ND, RMSK, is a naturopathic physician and registered musculoskeletal sonographer (RMSK) practicing at Regenerative Performance in Gilbert, AZ. He specializes in orthobiologic injections, including platelet-rich plasma, bone marrow concentrate, prolotherapy, perineural injection therapy, and nerve hydrodissection, using ultrasound and fluoroscopic guidance to treat the specific structures causing chronic pain rather than suppressing symptoms.
Dr. Timmermans has performed close to 10,000 orthobiologic injections, and contributes patient outcome data to the DataBiologics national registry to track responder rates and durability of treatment across thousands of cases.
References
- Kearney RS, Ji C, Warwick J, et al. Effect of Platelet-Rich Plasma Injection vs Sham Injection on Tendon Dysfunction in Patients With Chronic Midportion Achilles Tendinopathy (PATH-2): A Randomized Clinical Trial. JAMA. 2021;326(2):137-144. DOI: 10.1001/jama.2021.6986.
- Barreto ESR, Cruz ES, Antunes Junior CR, et al. Is Platelet-rich Plasma Effective in Treating Achilles Tendinopathy? A Meta-analysis of Randomized Clinical Trials. Clin Orthop Relat Res. 2024;483(5):779-790. DOI: 10.1097/CORR.0000000000003349.
- Radovanovic G, et al. Evidence-Based High-Loading Tendon Exercise for 12 Weeks Leads to Increased Tendon Stiffness and Cross-Sectional Area in Achilles Tendinopathy: A Controlled Clinical Trial. Sports Medicine - Open. 2022;8(1):149. DOI: 10.1186/s40798-022-00545-5.
- Bansal H, Leon J, Pont JL, et al. Platelet-rich plasma (PRP) in osteoarthritis (OA) knee: Correct dose critical for long term clinical efficacy. Sci Rep. 2021;11(1):3971. DOI: 10.1038/s41598-021-83025-2.
- Berrigan W, Tao F, Kopcow J, et al. The Effect of Platelet Dose on Outcomes after Platelet Rich Plasma Injections for Musculoskeletal Conditions: A Systematic Review and Meta-Analysis. Curr Rev Musculoskelet Med. 2024;17(12):570-588. DOI: 10.1007/s12178-024-09922-x.
NOTE: This article provides general information to help the reader better understand regenerative medicine, nerve and musculoskeletal conditions, naturopathic approaches to pain, and related subjects. All content provided in this article, website, or any linked materials, including text, graphics, images, research, and outcomes, are not intended, and should not be used, as a substitute for direct medical advice, diagnosis, or treatment. Please always consult with a professional and licensed healthcare provider to discuss if any treatment is right for you.
Registry data from our single practice, powered by DataBiologics, is not a randomized clinical trial. Individual results may vary.