
What Is Bioidentical Hormone Replacement Therapy in Gilbert, AZ?
Short Answer
- Bioidentical hormone replacement therapy (BHRT) uses hormones with the same molecular structure as the ones the body produces, prescribed individually for adults whose symptoms or labs point to a hormone imbalance, including women before, during, and after the menopausal transition and men with low testosterone
- Naturopathic BHRT in Gilbert begins with a workup tailored to the patient. For some patients that is a focused sex hormone panel; for others it includes the thyroid and adrenal systems alongside; the scope is chosen by Dr. Myers based on the picture in front of her, not a one-size-fits-all template
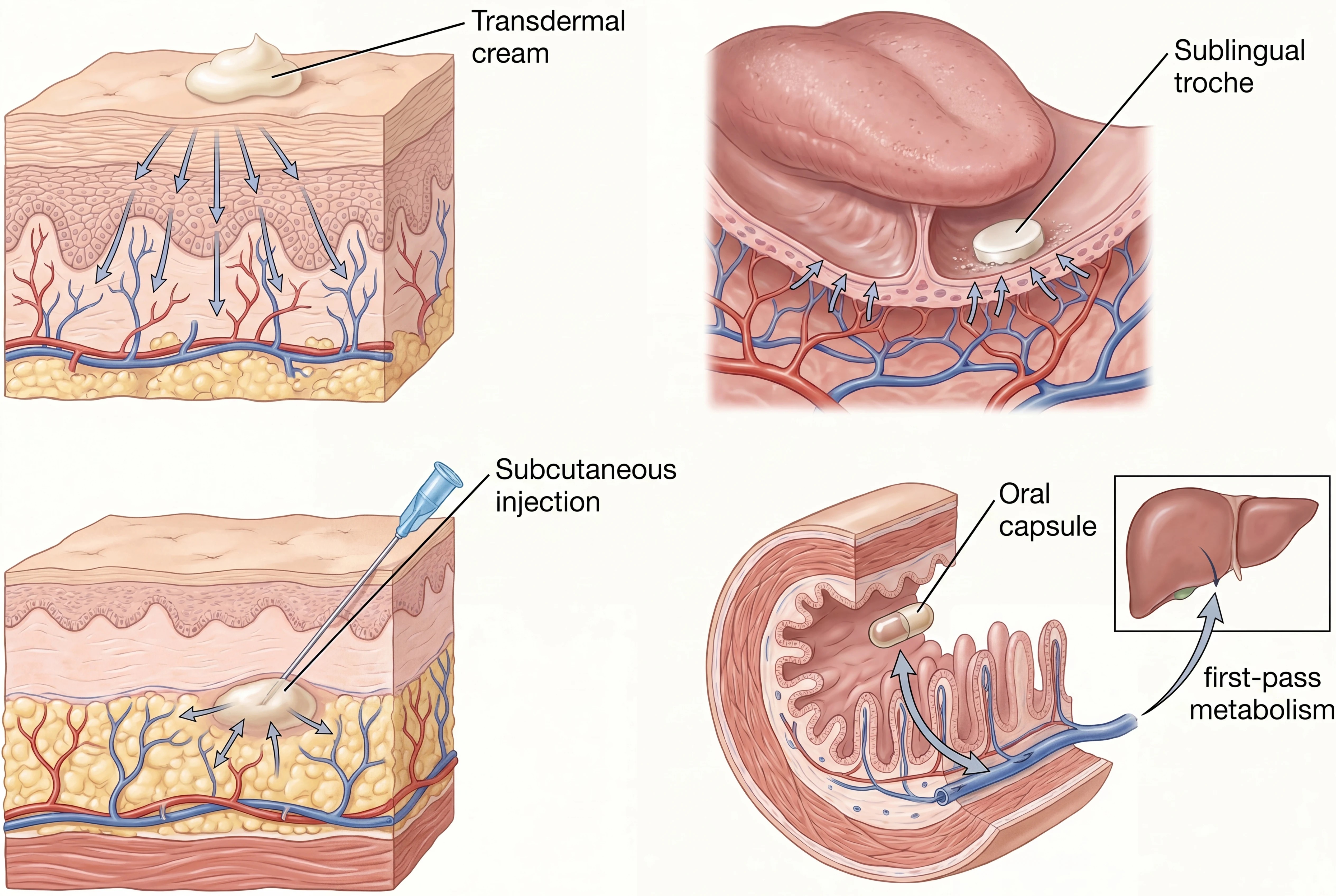
- Most patients notice meaningful symptom change within 6 to 12 weeks of an appropriately dosed regimen, with route of delivery (transdermal, oral, or injection) chosen based on individual risk factors and goals
Important note: BHRT decisions are individualized and require a licensed provider. Hormone therapy involves trade-offs that depend on personal and family history, current medications, age, and (for women) time since menopause. The information here is general patient education and is not a substitute for an evaluation. Bioidentical hormones include both FDA-approved formulations and compounded preparations, and both have a place when chosen carefully (ACOG Clinical Consensus No. 6, 2023).
If you have been told your labs are "normal" but you still feel exhausted, foggy, or out of sorts, the pattern is usually the same. You went to your primary care provider, asked about hormones, and were told the numbers looked fine, or were offered an antidepressant, or were sent home with a sleep aid. The missing step is almost always a workup designed for the specific question, with reference ranges interpreted in the context of your symptoms rather than in isolation. Sometimes that means looking at sex hormones in detail. Sometimes it means looking at thyroid, adrenal, and sex hormones together. Which version is right depends on the patient.
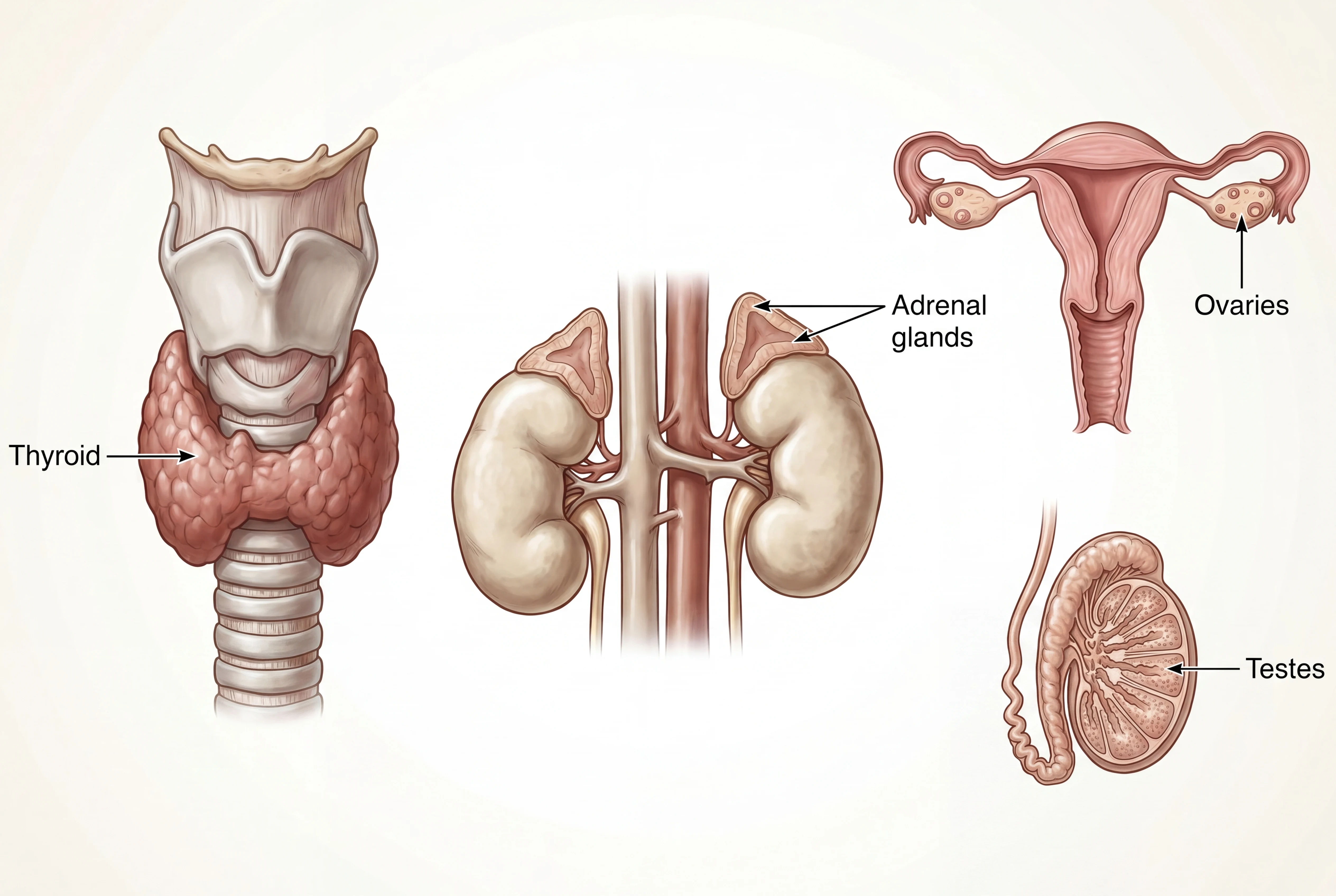
Bioidentical hormone replacement therapy is a treatment approach that uses sex hormones (estradiol, progesterone, testosterone, DHEA) with a molecular structure matching the hormones the body already produces. When the workup indicates, bioidentical thyroid hormone (such as desiccated thyroid, T3, or T4) and bioidentical adrenal support may be prescribed alongside as part of integrated hormone care. The goal is to restore physiologic levels in patients whose own production has declined, and to do it with formulations and routes of delivery that minimize known risks.
At Regenerative Performance in Gilbert, Arizona, hormone care is led by Dr. Kaitlyn Myers, a naturopathic physician who works with women across the full hormonal arc (PMS and cycle issues, perimenopause, menopause, and post-menopause), with men whose energy, libido, mood, body composition, or sleep point to a testosterone problem, and with patients whose thyroid or adrenal patterns are contributing to symptoms that BHRT alone will not resolve. The workup happens before the prescription, not after.
This article covers what BHRT is, how a naturopathic approach differs from the high-volume hormone clinic model, who is and is not a candidate, what the first visit looks like, and what hormone options we use most often.
If you have hormone symptoms that have not responded to previous treatments, or if your current hormone protocol is not getting you where you want to be, the next step is a comprehensive evaluation that maps your full hormone picture before any prescription is written or adjusted.
Schedule a comprehensive evaluation for your hormone health at our Gilbert, AZ clinic (also serving Chandler, Mesa, Queen Creek, and the greater Phoenix area).
Key Facts About Naturopathic BHRT
- What BHRT is: A prescription approach using bioidentical sex hormones (estradiol, progesterone, testosterone, DHEA) that match the molecular structure of endogenous hormones. When the workup indicates, bioidentical thyroid hormone and bioidentical adrenal hormones are prescribed alongside as part of integrated hormone care
- Who it helps: Women before, during, or after the menopausal transition with vasomotor, sleep, mood, or genitourinary symptoms. Men with documented low testosterone and matching symptoms. Selected patients with thyroid or adrenal dysfunction contributing to the picture
- How a naturopathic workup differs: Lab panel selected for the specific clinical question (sometimes focused, sometimes broad), evaluated alongside symptoms, sleep, stress, gut, and nutrient status. Route of delivery chosen by risk profile rather than clinic default
- Goal of treatment: Restore physiologic hormone levels, reduce symptom burden, and address upstream contributors so dosing can stay conservative
- Timeline: Many patients notice meaningful change in 6 to 12 weeks; full benefit is typically reached by 3 to 6 months with dose titration along the way
- Where: Regenerative Performance, Gilbert, AZ; serving Mesa, Chandler, Queen Creek, Scottsdale, and the greater Phoenix area
- Next step: Call 480-508-4226 to schedule a comprehensive evaluation for your hormone health
What Is Bioidentical Hormone Replacement Therapy?
Bioidentical hormone replacement therapy is hormone therapy that uses molecules identical in structure to the ones produced by the human body. The most commonly prescribed are 17-beta estradiol, estriol, micronized progesterone, testosterone, and DHEA. The defining feature is structure, not source. A bioidentical hormone can be FDA-approved (manufactured by a pharmaceutical company in standardized doses) or compounded (mixed by a licensed compounding pharmacy to a custom dose or formulation).
This is the most common point of confusion. Patients hear "bioidentical" and assume it means "compounded only," or assume it means "natural and therefore safer." Neither is quite right.
Bioidentical vs synthetic: structure, not source
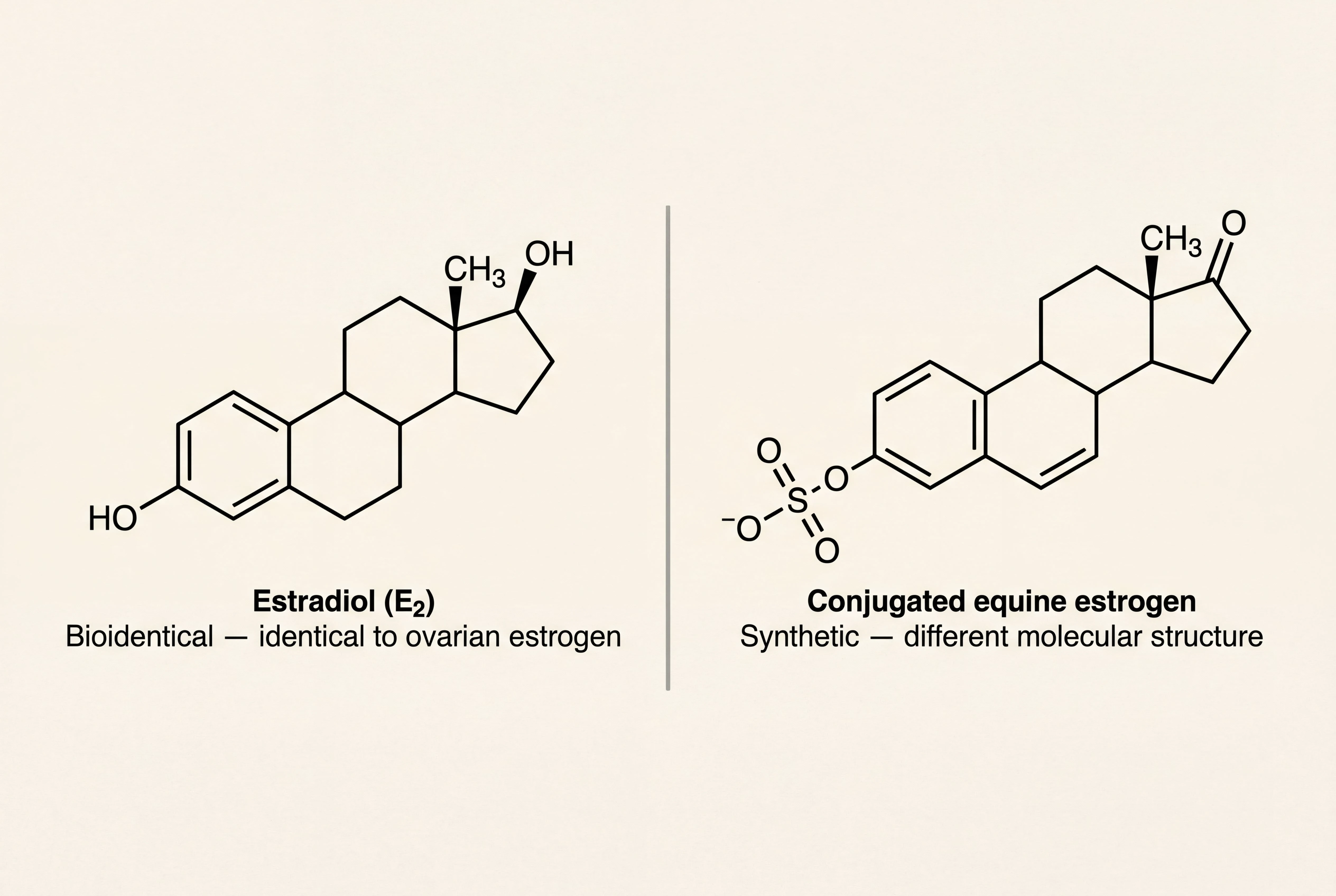
Synthetic hormones used in older HRT regimens (for example, conjugated equine estrogens or medroxyprogesterone acetate) have a different molecular structure than the hormones the human body makes. The body responds to them through similar receptor pathways, but with a different downstream profile. Modern menopausal hormone therapy increasingly favors bioidentical formulations because of more predictable receptor binding and a better-studied safety profile in several populations (Flores VA, et al., Endocrine Reviews, 2021).
Compounded vs FDA-approved
The American College of Obstetricians and Gynecologists 2023 clinical consensus on compounded BHRT clarifies the practical decision tree. FDA-approved bioidentical estradiol (oral and transdermal), bioidentical progesterone (oral micronized), and combination products are appropriate first-line options for many patients because they have predictable potency, established dosing, and broad evidence (ACOG Clinical Consensus No. 6, 2023). Compounded formulations earn a place when an FDA-approved option is not available at the dose a patient needs, when a patient has an allergy to an inactive ingredient in a manufactured product, or when a less common combination is clinically warranted.
Because we practice personalized medicine, most patients in our practice receive compounded preparations. That lets us tailor the dose and the delivery system to exactly what the patient needs rather than defaulting to a manufactured strength that may not be the right fit. As one example, many men on commercial testosterone replacement react to the carrier oil used in the FDA-approved injection. We often prescribe compounded testosterone in a different carrier (such as MCT oil), which appears to produce fewer of those reactions. Compounding is a clinical tool, not a marketing tagline, and the decision to use it is made case by case.
How a Naturopathic Approach to BHRT Differs
A naturopathic approach to BHRT begins with a workup tailored to the patient, then chooses the formulation, dose, and route of delivery that fit both the workup and the patient's preferences. The contrast with a pellet-first clinic for women or a high-volume TRT clinic for men is not whether labs are run (most reputable clinics order labs), but in three specific places: dosing flexibility, what gets evaluated alongside the sex hormones, and what gets done in parallel with hormone replacement to make the hormones work.
Dosing flexibility (and why we do not use pellets)
For women, a pellet locks a patient into a dose for several months because the pellet is implanted and releases hormone over that time. If the dose turns out to be too high (over-suppression, side effects, mood changes) or too low (incomplete symptom relief), the patient is committed to that dose until the pellet wears off. We prefer formulations that allow real-time titration based on labs and clinical response, so the dose can move with the patient rather than the patient waiting on a pellet to clear.
For men, the comparable issue at high-volume TRT clinics is protocol-style dosing, which means pushing testosterone to the upper end of the reference range and routinely co-prescribing aromatase inhibitors like anastrozole regardless of estradiol levels, rather than dosing for the individual patient and titrating against response. Many men come to us specifically because the high-dose-plus-anastrozole template did not produce the result they were looking for, or did but with downstream issues.
What gets evaluated alongside sex hormones
Many TRT and pellet clinics use protocol-style dosing without individualizing for the upstream contributors that affect hormone status. Sex hormone levels can be influenced by sleep, stress, nutrition, gut function, blood sugar, body composition, life stage, and (when relevant) thyroid and adrenal function. A patient whose testosterone is low because of poor sleep and chronic stress may not need testosterone replacement at all once those upstream contributors are addressed. A patient whose perimenopausal symptoms are layered on top of underlying thyroid dysfunction needs both addressed in parallel.
The labs we run on a first BHRT visit reflect that picture-first approach, and the exact panel depends on the clinical question. For some patients that means a focused sex hormone panel. For others it means a sex hormone panel alongside the thyroid panel (TSH, free T3, free T4, reverse T3, antibodies), the adrenal panel (often a four-point salivary or urinary cortisol), and selected nutrient and metabolic markers. The goal is to evaluate enough to make a good decision, not to run every test on every patient.
This matters because hormone systems do not move in isolation. When one system is treated, the others tend to shift, which is why our follow-up cadence includes retesting other endocrine markers periodically rather than only the system we are dosing. A patient whose thyroid hormone is increased without parallel attention to adrenal output will sometimes feel worse before they feel better, because the adrenals cannot keep up with the metabolic demand a higher thyroid dose creates.
What gets done alongside hormones to make hormones work
The naturopathic side of BHRT is not the prescription. The prescription is the easy part. The harder and more impactful part is the parallel work that makes the hormones do their job: nutrition adapted to insulin sensitivity and body composition, targeted supplementation for cofactors the labs flag (vitamin D, magnesium, B12, iron, methylation support), sleep and stress protocols, structured exercise (resistance training is non-negotiable for both BHRT and TRT patients), and selective use of peptide therapy where the clinical picture supports it. A patient on the right dose of estradiol with poor sleep, no resistance training, and a diet that spikes blood sugar will not feel the way the dose is supposed to make them feel. A patient with the same prescription whose lifestyle and supplement layer is dialed in will.
This is the through-line of naturopathic medicine: address the upstream contributors first, then add the hormone, then track the result.
Shared decision-making and dose titration
The first prescription is rarely the right long-term prescription. Dosing is titrated based on response, on follow-up labs, and on whether the underlying contributors (sleep, stress, blood sugar, gut function, nutrient status) are being addressed in parallel. A patient who improves on a starting dose but does not get all the way there often needs the upstream pieces tightened up before the dose is escalated.
Route of delivery matters
This is the area where many BHRT clinics and patients are operating on outdated information. Not all routes of delivery carry the same risk profile.
A 2019 nested case-control study in BMJ analyzed more than 80,000 women in two large UK databases and found that oral estrogen significantly increased venous thromboembolism (VTE) risk while transdermal estrogen showed no measurable increase in VTE risk over baseline (Vinogradova Y, et al., BMJ, 2019). A 2021 review in the Journal of Clinical Endocrinology & Metabolism reinforced that route of delivery and formulation are central to cardiovascular risk decisions, not afterthoughts (Shufelt CL, Manson JE, JCEM, 2021).
In our practice, transdermal estradiol is strongly preferred over oral, and we do not use oral estrogen because of the documented thrombotic and stroke risks. Creams, patches, and injections each have their place; pellets carry the dose-flexibility limitation noted earlier, so we do not use them either.
Who Is a Candidate for BHRT?
BHRT is appropriate for several patient profiles. It is not appropriate for everyone, and that distinction is one of the most important parts of the workup.
Perimenopause (often the 40s)
Perimenopause typically starts in the early to mid 40s and lasts an average of 4 to 8 years before final menstruation. The pattern is irregular cycles, sleep that becomes broken without an obvious reason, mood changes that do not match life circumstances, hot flashes that come and go, and changes in libido, weight, or cognition. Hormones in perimenopause swing rather than fall in a straight line, which is part of why a single lab snapshot can miss what is actually happening.
Candidates for BHRT in perimenopause are women whose symptoms are interfering with sleep, work, relationships, or daily function, and whose workup confirms that hormonal change is a meaningful contributor.
Menopause and post-menopause
Once a woman has gone 12 consecutive months without a period, she is considered post-menopausal. The vasomotor symptoms (hot flashes, night sweats), genitourinary symptoms (vaginal dryness, urinary urgency), bone density loss, and changes in cardiovascular risk after menopause are all influenced by the loss of endogenous estrogen.
The American Heart Association's 2020 scientific statement on the menopause transition makes the case for what is sometimes called the timing hypothesis: starting hormone therapy in early menopause (typically within 10 years of menopause onset, or before age 60) carries a different cardiovascular risk profile than starting it 20 years later. The transition itself is a window where intervention has more leverage, and where decisions about hormone therapy should be made with that window in mind (El Khoudary SR, et al., Circulation, 2020).
Candidates for BHRT in menopause and post-menopause are women whose vasomotor symptoms, sleep disruption, genitourinary changes, mood changes, or bone density concerns are interfering with quality of life, particularly when the workup is happening within the timing-hypothesis window. The earlier the workup happens after menopause, the more options remain on the table.
Men with low or low-normal testosterone and matching symptoms
In men, testosterone replacement is appropriate when symptoms (low energy, low libido, mood change, loss of muscle mass, harder-to-shift body fat, sleep disruption) line up with the lab picture. The reference range bottom for total testosterone is set very low, so a number that the lab calls "normal" can still be low enough to drive real symptoms. A meaningful percentage of men we work with come in with testosterone in the lower portion of normal rather than below it, and we treat against the symptom-and-lab picture rather than waiting for the number to fall further.
A naturopathic workup includes a full panel (total and free testosterone, SHBG, estradiol, prolactin, complete blood count, lipids, and metabolic markers) before a decision is made. We also screen for the upstream contributors that suppress testosterone, because resolving those sometimes reduces (or eliminates) the need for replacement.
Candidates for testosterone replacement at our practice are men whose symptom-and-lab picture supports it AND who are committed to the parallel work (sleep, training, nutrition, stress) that keeps the dose conservative and the result durable.
Women and testosterone
Testosterone is not only a male hormone. The International Society for the Study of Women's Sexual Health 2021 clinical practice guideline supports systemic testosterone for postmenopausal women with hypoactive sexual desire disorder (HSDD) when other contributors have been addressed (Parish SJ, et al., J Sex Med, 2021). Doses for women are roughly one-tenth of male doses, with monitoring of total testosterone, free testosterone, and clinical response.
Candidates for systemic testosterone in women are typically post-menopausal patients with HSDD or low libido that has not responded to addressing other contributors first (sleep, stress, the estrogen and progesterone side of the workup, relationship and life-stage factors). Testosterone in women is rarely the only intervention; it is one piece of a fuller picture.
When BHRT is NOT appropriate
There are situations where hormone therapy is contraindicated or carries enough risk that the answer is no:
- Active or recent hormone-sensitive cancer (breast, endometrial, certain ovarian cancers)
- A recent venous thromboembolism, pulmonary embolism, or stroke
- Pregnancy or active breastfeeding
- Undiagnosed abnormal uterine bleeding
- Severe active liver disease
A history of one of these does not always close the door permanently, but it does change the conversation. A workup that surfaces these factors before a prescription is written is the workup we run.
What the First Visit Looks Like at Regenerative Performance
The first BHRT visit at our Gilbert clinic is built around getting the picture right.
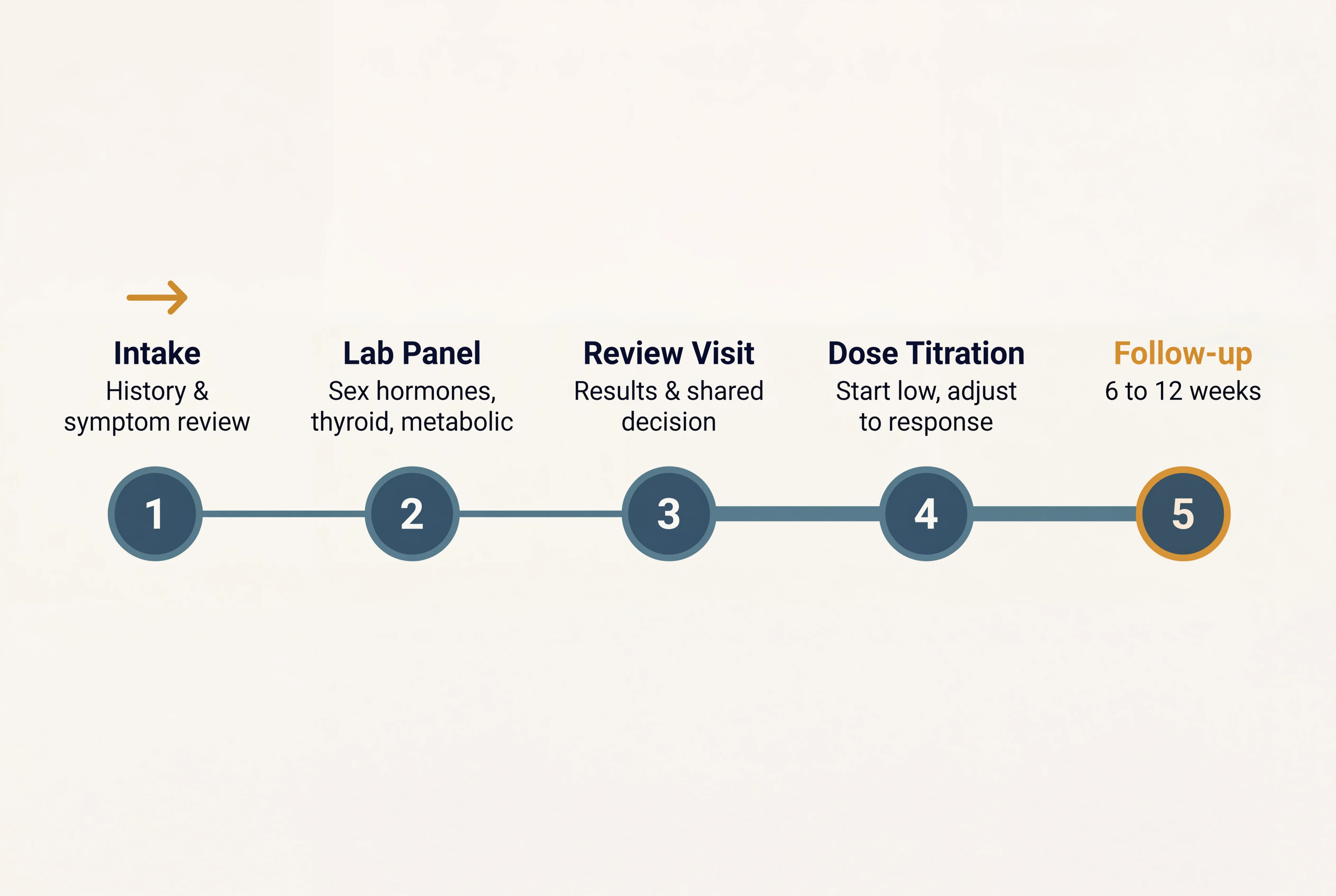
The intake covers your symptoms, current and past medications, prior hormone therapy if any, surgical history, family history (with attention to cancer and clotting), sleep, stress, gut function, nutrient intake, and what you have already tried. We ask about how mornings feel, how energy moves through the day, how sleep breaks down, and what the cycle (if you still have one) is doing.
The lab panel ordered on a first visit is broader than what most patients have had before. It typically includes a full sex hormone panel, the full thyroid panel including reverse T3 and antibodies, a four-point cortisol if the pattern suggests adrenal involvement, fasting metabolic markers, and selected nutrients (vitamin D, B12, ferritin, magnesium where indicated).
A review visit walks through the labs in the context of what you reported at intake. The plan that comes out of that review is shared, not handed down. We discuss which formulation, which route, and which dose make sense for you given your risk profile and goals, and we agree on what change you should expect by the next follow-up.
Follow-up cadence depends on the regimen. Early in therapy, follow-up is typically at 6 to 12 weeks with repeat labs and dose adjustment. Once a stable dose is reached, lab monitoring moves to every 6 months for a year, then annually. Visit cadence with Dr. Myers typically remains every 3 months or so during that time, because she is also working on the other aspects of your health (sleep, stress, nutrition, gut function, exercise, supplements) from a naturopathic standpoint. The hormone is one input; the full plan is what produces the durable result.
If you are unsure whether BHRT is right for your situation, or you are traveling from outside the Phoenix area, you can also call 480-508-4226 and ask about a brief 15 minute discovery call.
Schedule a comprehensive evaluation for your hormone health at our Gilbert, AZ clinic.
Bioidentical Hormone Options We Prescribe
The formulations and routes used most often in naturopathic BHRT, with the clinical reasoning for each:
Estradiol and estriol (compounded E2/E3 cream is our default)
In our practice, Dr. Myers typically prescribes a compounded estradiol-and-estriol (E2/E3) cream rather than a single-hormone patch or an oral product. The compounded E2/E3 cream allows precise dosing flexibility that fixed patch strengths do not, and estriol contributes its own clinical benefits (cervical and vaginal tissue support, less proliferative signaling than estradiol alone) that the patient does not get from estradiol in isolation.
We do not use oral estrogen because of the documented thrombotic and stroke risks discussed above. Patients coming to us are typically seeking to avoid those risks specifically, and the transdermal compounded cream lets us deliver bioidentical estrogen support without the first-pass liver burden that drives the oral risk profile.
Micronized progesterone (oral, bedtime)
Women with an intact uterus on estrogen require progesterone to protect the endometrial lining. Oral micronized progesterone has two advantages worth knowing. First, it has a documented endometrial protective effect when dosed appropriately. Second, it has a clinically useful sleep benefit when taken at bedtime. A 2021 systematic review and meta-analysis of randomized controlled trials in JCEM found that oral micronized progesterone improved sleep quality in peri- and postmenopausal women (Nolan BJ, et al., JCEM, 2021). Synthetic progestins do not share this profile.
Testosterone (men and women, different doses)
For men, testosterone is delivered as injection or transdermal cream in our practice, with dose targeted to a physiologic range and monitored over time. (We do not use pellets for the dosing-flexibility reasons discussed earlier.) For women with HSDD, dosing is roughly one-tenth of a male dose with monitoring as described above.
DHEA and thyroid support when indicated
DHEA is added when adrenal labs and clinical picture support it, particularly in women with low DHEA-S and symptoms of fatigue or low libido that are not fully responding to estrogen and progesterone alone. Bioidentical thyroid hormone, when indicated, may be desiccated thyroid or selective T3 and T4 dosing. We titrate carefully against clinical markers (including morning resting pulse rate, where a 30 percent rise from baseline can signal that we are pushing into hyperthyroid range) rather than relying on TSH alone, which can lag clinical change by weeks.
Common Questions Patients Ask
Is bioidentical hormone replacement therapy safer than traditional HRT?
Bioidentical hormones used in current FDA-approved formulations and dosed at physiologic levels have a well-studied safety profile in most populations, particularly when route of delivery is matched to risk factors. Compounded BHRT is appropriate when an FDA-approved option does not fit, but is not automatically safer than a manufactured equivalent. The risk question is always specific to the formulation, the dose, and the patient's history (ACOG, 2023; Flores et al., 2021).
Who is a candidate for BHRT in Gilbert?
Women in perimenopause or menopause with symptoms interfering with daily function, men with documented low testosterone and matching symptoms, and selected patients with thyroid or adrenal dysfunction. Candidacy is confirmed by a workup that maps the full hormonal picture, not by symptoms alone.
What testing does Dr. Myers order before starting BHRT?
A full sex hormone panel, full thyroid panel including reverse T3 and antibodies, a four-point cortisol when indicated, fasting metabolic markers, and selected nutrient labs. The goal is a workup that lets us see how the systems are interacting, not just the level of one hormone in isolation.
How long does it take to feel better on BHRT?
Many patients notice meaningful change within 6 to 12 weeks of an appropriately dosed regimen. Full benefit is typically reached by 3 to 6 months with dose titration along the way. Patients who also work on the upstream contributors (sleep, stress, blood sugar, gut, nutrient status) often see broader improvement than hormones alone produce.
What is the difference between creams, patches, injections, and pellets?
Creams and patches deliver transdermal estradiol with the lower VTE risk profile observed in large cohort data. Injections allow precise dose titration for testosterone in men and can be self-administered or given in office. Pellets release hormone at a relatively steady rate over 3 to 5 months but cannot be adjusted or removed if a side effect develops, so we do not use them in our practice. The right route is the one that matches your risk profile and your follow-up cadence.
Can men get BHRT at Regenerative Performance, or is it just for women?
BHRT at Regenerative Performance serves both men and women. Dr. Myers works with men whose energy, libido, mood, body composition, or sleep point to a testosterone problem (including men whose labs are technically "normal" but on the low end), alongside her work with women across the full hormonal arc, including perimenopause, menopause, post-menopause, and earlier hormone-related cycle or symptom issues. The workup framework is the same: full panel sized to the clinical question, root contributors first, then prescription.
I had breast cancer in the past. Can I still consider BHRT?
Sometimes, but the conversation is more involved. Active or recent hormone-sensitive cancer is a contraindication to systemic estrogen. A more distant history may allow consideration of selected formulations (for example, vaginal estrogen for genitourinary symptoms) after coordination with your oncology team. The answer is specific to your history and warrants a careful evaluation rather than a yes or no over the phone.
How is naturopathic BHRT different from what a Biote-certified clinic offers?
The difference is in two places: dosing flexibility and what gets evaluated alongside the sex hormones. A pellet locks the patient into a single dose for several months, which is the dosing-flexibility limitation that keeps us from using pellets in our practice. A high-volume pellet or TRT clinic also tends to use protocol-style dosing without individualizing for the upstream contributors that affect hormone status. A naturopathic workup looks at the picture in front of the patient (sex hormones in detail, sometimes alongside thyroid, adrenal, and metabolic markers), addresses upstream contributors, and chooses the formulation and route based on that picture rather than a default protocol.
Will I need to be on BHRT forever?
Not necessarily. The goal is to support a patient through symptoms and a window of risk where hormone replacement adds clinical value. Dose can be reduced over time, and some patients taper off after symptoms resolve and lifestyle and upstream contributors are stable. Long-term use is appropriate for some patients and is reviewed with you at each follow-up.
Still have questions? The best way to get answers is a conversation. Call 480-508-4226.
Getting Started in Gilbert, Mesa, Chandler, and the East Valley
Naturopathic BHRT is a long-term relationship more than a single transaction. The first visit is the longest because it sets up everything that follows.
What to bring to your first visit: a list of current medications and supplements, copies of any prior hormone or thyroid labs you have, and a written sense of what is bothering you most and what change you are hoping for. The second item is more important than it sounds; clarity about goals lets us measure progress against something specific rather than vague wellness.
Dr. Myers leads BHRT, women's health, and men's hormone care at Regenerative Performance, and works alongside Dr. Drew Timmermans on patients whose hormone picture intersects with chronic musculoskeletal pain or recovery. The two sides of the practice complement each other where they overlap, and hormone care across both men and women is led by Dr. Myers.
About Dr. Kaitlyn Myers

Dr. Kaitlyn Myers, ND
Dr. Kaitlyn Myers is a naturopathic physician at Regenerative Performance in Gilbert, AZ. She leads the practice's hormone therapy, functional medicine, and internal medicine care. She works with women across the full hormonal arc and with men whose testosterone and metabolic picture warrant attention, treats thyroid and adrenal dysfunction, resolves chronic infections such as Lyme and mold toxicity, and uses comprehensive functional labs to uncover root causes. Dr. Myers is a graduate of Southwest College of Naturopathic Medicine in Tempe, Arizona, and practices an investigative, systems-based approach to complex chronic illness.
References
- Pinkerton JV, et al. Compounded Bioidentical Menopausal Hormone Therapy: ACOG Clinical Consensus No. 6. Obstetrics & Gynecology. 2023;142(5):1266-1273. DOI: 10.1097/AOG.0000000000005395.
- Vinogradova Y, Coupland C, Hippisley-Cox J. Use of hormone replacement therapy and risk of venous thromboembolism: nested case-control studies using the QResearch and CPRD databases. BMJ. 2019;364:k4810. DOI: 10.1136/bmj.k4810.
- Flores VA, Pal L, Manson JE. Hormone Therapy in Menopause: Concepts, Controversies, and Approach to Treatment. Endocrine Reviews. 2021;42(6):720-752. DOI: 10.1210/endrev/bnab011.
- Shufelt CL, Manson JE. Menopausal Hormone Therapy and Cardiovascular Disease: The Role of Formulation, Dose, and Route of Delivery. J Clin Endocrinol Metab. 2021;106(5):1245-1254. DOI: 10.1210/clinem/dgab042.
- El Khoudary SR, et al. Menopause Transition and Cardiovascular Disease Risk: Implications for Timing of Early Prevention: A Scientific Statement From the American Heart Association. Circulation. 2020;142(25):e506-e532. DOI: 10.1161/CIR.0000000000000912.
- Nolan BJ, Liang B, Cheung AS. Efficacy of Micronized Progesterone for Sleep: A Systematic Review and Meta-analysis of Randomized Controlled Trial Data. J Clin Endocrinol Metab. 2021;106(4):e942-e951. DOI: 10.1210/clinem/dgaa873.
- Parish SJ, Simon JA, Davis SR, et al. International Society for the Study of Women's Sexual Health Clinical Practice Guideline for the Use of Systemic Testosterone for Hypoactive Sexual Desire Disorder in Women. J Sex Med. 2021;18(5):849-867. DOI: 10.1016/j.jsxm.2020.10.009.
NOTE: This article provides general information to help the reader better understand bioidentical hormone replacement therapy, naturopathic approaches to hormone health, and related subjects. All content provided in this article, website, or any linked materials, including text, graphics, images, research, and outcomes, are not intended, and should not be used, as a substitute for direct medical advice, diagnosis, or treatment. Hormone therapy decisions are individualized and require evaluation by a licensed provider. Please always consult with a professional and licensed healthcare provider to discuss if any treatment is right for you.