PRP for SI Joint Pain: What the Evidence Shows
Short Answer
- PRP (platelet-rich plasma) injections can help adults with chronic low back pain that originates from the sacroiliac joint.
- PRP uses concentrated growth factors from your own blood, placed under ultrasound and/or fluoroscopic guidance, into the sacroiliac joint and specific sacroiliac ligaments that are generating the pain.
- Roughly three out of four low-back and SI joint patients in our registry report significant pain relief by 12 months.
For adults in Mesa, Gilbert, and Apache Junction who have been told their low back pain is a disc problem or sciatica but the treatments based on those diagnoses have not worked, the pattern is common: the pain may be coming from the sacroiliac joint, a structure that most providers do not properly evaluate as a cause of low back pain.
If you have chronic low back pain, the pattern is usually the same: physical therapy helped for a while, cortisone gave only temporary relief, your MRI showed a disc issue but treatments have not helped, and surgery is now on the table. Many of our patients arrive with this exact history, but once the structures actually generating the pain are identified and treated directly, pain and function usually improve.
PRP injections for sacroiliac joint pain are a non-surgical, injection-based treatment that uses concentrated growth factors from your own blood to support tissue repair in the SI joint and surrounding ligaments. At Regenerative Performance in Gilbert, AZ, we use ultrasound and x-ray guidance to target each pain-generating structure directly rather than placing a single injection into the joint space and hoping it covers everything. This approach is most appropriate after conservative care has not helped and when a thorough physical examination confirms the SI joint is the source. PRP for SI joint pain is typically not covered by insurance, and results vary by patient.
If you have chronic low back pain that has not improved with physical therapy, chiropractic, or cortisone, the next step is a detailed, in-person assessment to identify the exact tissues causing your pain and review non-surgical orthobiologic options like PRP and stem cell therapy.
Schedule a comprehensive 2-hour evaluation for your chronic low back pain at our Gilbert, AZ clinic (also serving Mesa, Apache Junction, Chandler, and the greater Phoenix area).
At our Gilbert, AZ clinic serving Mesa, we use ultrasound and x-ray-guided PRP as a non-surgical treatment option for sacroiliac joint pain, allowing patients to often avoid an indefinite cycle of cortisone or surgery when those are not addressing the real pain source. In our clinic, we most often see active adults 40 and older whose MRI reports do not explain their pain, and whose symptoms respond once the sacroiliac joint and supporting ligaments are properly evaluated and treated directly under ultrasound and/or x-ray guidance.
Key Facts About PRP for SI Joint Pain
Here is what you need to know about PRP for SI joint pain before deciding whether it is worth exploring.
- What PRP is: Platelet-rich plasma (PRP) is a preparation concentrated from your own blood that delivers a high dose of growth factors and platelets directly into the damaged sacroiliac ligaments and joint around the pelvis.
- Who it helps: Adults with chronic low back, hip, or leg pain originating from the SI joint and sacroiliac ligaments that has not improved with physical therapy, chiropractic care, or cortisone injections, particularly when the pain started after an injury, pregnancy, or gradually worsened without a clear explanation.
- How it works: Under ultrasound and x-ray guidance, PRP is injected into the specific sacroiliac ligaments that are lax or damaged, the SI joint, and any other connective-tissue pain generators identified on physical exam.
- Clinical outcomes: Low-back and SI joint cases in our registry see 74% of patients reporting significant pain relief at 12 months. Among the 109 cases with completed safety follow-up in our registry, zero severe treatment-related adverse events have been recorded, in registry data collected over more than 5 years.
- Timeline: Most patients begin to notice a reduction in pain within 4 weeks, with most improvement occurring over the first 3 months. Some patients continue to improve for 6 to 9 months, and results can last >2 years. Individual results may vary.
- Typical treatments: We start with one PRP session and track your individual response. A second session is considered 12 weeks later based on how you responded. Blood draw volume of 120 to 300 mL, significantly larger than the 60 mL or less used at most clinics, to support proper platelet dosing.
- Where: Regenerative Performance, a regenerative and interventional orthobiologic clinic in Gilbert, AZ, serving patients from the greater Phoenix area including Mesa.
- Next step: Call 480-508-4226 to schedule a 2-hour evaluation for SI joint pain in Gilbert, AZ.
This page is especially useful if you have been diagnosed with a disc bulge, sciatica, or degenerative disc disease, the treatments based on those diagnoses have not helped, and you live in or near Mesa, AZ.
What Causes SI Joint Pain That Is Not Coming from Your Spine?
SI joint pain that is not coming from your spine is usually caused by lax, damaged, or irritated ligaments supporting the sacroiliac joint, which allow abnormal motion that generates pain. It is one of the most commonly overlooked sources of chronic low back pain because conventional imaging doesn't show SI ligament injuries well, and it can generate pain that looks like sciatica on a symptom list but has nothing to do with the sciatic nerve or a lumbar disc.
When someone comes in with chronic low back pain that has not responded to treatment, we evaluate a structure that conventional providers frequently overlook.
The Sacroiliac (SI) Joint
The sacroiliac joint (the joint where your sacrum, the triangular bone at the base of your spine, meets your ilium, or pelvis) is a frequently overlooked contributor to chronic low back pain in conventional care. A 2009 study in Spine by Sembrano and Polly, and a 2013 review by Cohen and colleagues in Expert Review of Neurotherapeutics, suggest the SI joint contributes to an estimated 15 to 30 percent of chronic low back pain cases, yet many providers never test for it. SI joint dysfunction occurs when the ligaments holding this joint stable become lax or irritated, allowing abnormal motion that generates pain.
SI joint pain can be challenging to diagnose as the pain does not always stay just in the low back. SI joint dysfunction can refer pain into the back of the hip, the front of the groin, and even down the leg into the calf or foot. Many patients with SI joint problems have been told they have sciatica, because the pain travels down the leg, but the sciatic nerve is not involved. The pain is coming from the SI joint and its ligaments, and when those structures are treated, the "sciatica" often resolves.
One of the most reliable clues that the SI joint may be involved is pain with transitions. If going from sitting to standing, getting in and out of the car, or rolling over in bed reproduces your pain, the SI joint should be evaluated.
What Is PRP Treatment for SI Joint Pain?
PRP (platelet-rich plasma) treatment for SI joint pain is a non-surgical, injection-based approach that uses your own blood to support tissue repair in the SI joint and its surrounding ligaments.
Rather than numbing the pain temporarily with cortisone or ablating nerves to block the signal, PRP delivers concentrated growth factors to the damaged structures to support actual healing.
How Do PRP Injections Work for SI Joint Pain?
PRP injections work for SI joint pain by delivering concentrated growth factors directly into the damaged ligaments and joint, where they support tissue repair and reduce the inflammation driving chronic pain. Under ultrasound guidance for the ligaments and ultrasound and x-ray for the joint itself, we treat each pain-generating structure individually rather than blindly injecting near the joint space.

Growth Factor Concentration and Delivery
PRP is concentrated from your own blood, which means the volume of blood we draw matters. At Regenerative Performance we typically draw 120 to 300 mL, compared to the industry norm of 60 mL or less, and that larger draw gives us a higher dose of platelets and growth factors per injection. We target a platelet concentration of 5 to 20 times baseline, ensuring that we are achieving optimal platelet dosing for each specific injection site. It is similar to taking one-eighth of a Tylenol for a headache: if the headache does not improve, the problem is not Tylenol, it is the dose. Underdosed PRP is one of the most common reasons patients tell us they have already tried it and it did not help.
Ligament Repair and SI Joint Stability
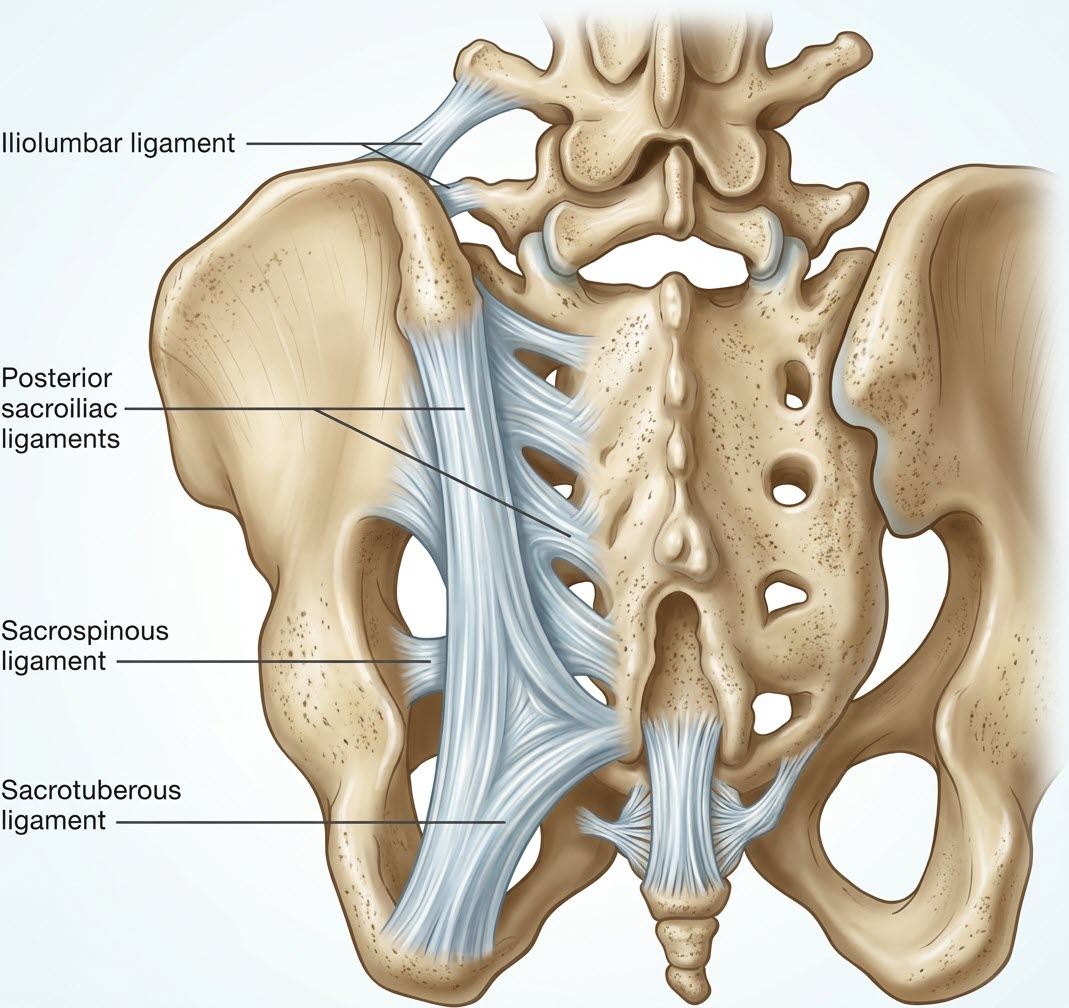
If you have sacroiliac joint dysfunction, most of the pain is actually coming from the ligaments outside the joint, not the joint space itself. The posterior sacroiliac ligament, the interosseous ligament, and the long dorsal sacroiliac ligament all stabilize the joint, and all of them can become lax or damaged after an injury, pregnancy, or years of mechanical stress. Instead of placing a single injection into the SI joint and hoping it covers everything, we use ultrasound to identify the specific ligaments that are damaged and treat each one directly, along with the joint itself when the imaging and physical exam point there. That structure-by-structure approach is a big reason our outcomes hold up in cases where a single joint-space injection has already been tried and failed.
Inflammation Modulation
In chronic SI joint dysfunction, the inflammation around lax ligaments stops being protective and starts driving the pain cycle itself. The growth factors in PRP shift that environment in a way that supports repair rather than just quieting the signal. Patients often describe the change as a slow, steady reduction over weeks rather than an immediate numbing effect, which honestly makes sense, because the tissue is actually doing something rather than just having its pain receptors turned down. That is a really different experience from a cortisone injection, where the relief can be fast but the ligament damage is still there.
Pain Signal Reduction
Once the ligaments stabilize, the joint stops generating the chronic pain signal, and patients usually notice the shift gradually over 3 to 6 months. This feels different from medication-based relief because the underlying source is being treated rather than the signal masked, which is why the improvement tends to hold even after the treatment course ends.
Important note: In the United States, PRP for sacroiliac joint pain is typically an off-label use of devices cleared to prepare platelet concentrates, not an FDA-approved treatment for sacroiliac joint dysfunction. We use PRP as a cash-pay option after conservative care has not helped. Results vary from person to person.
Early clinical research on PRP for the SI joint is still building. A 2017 pilot study by Singla and colleagues showed meaningful short-term improvements in pain and function in patients with sacroiliac joint dysfunction, which matches what we see in our own practice when the diagnosis is right and the injection is image-guided. Larger controlled trials are still needed, and that is an honest limitation of where the research stands right now.
Outcome Snapshot
Our patient outcome registry tracks lumbosacral and pelvis cases as a body region, which includes sacroiliac joint dysfunction along with other low back and pelvic pain generators. At 12 months, 74% of patients in this cohort report significant pain relief, and 77% report relief at 18 months. Among the 109 cases with completed safety follow-up in our registry, zero severe treatment-related adverse events have been recorded, in registry data collected over more than 5 years.
Schedule a comprehensive 2-hour evaluation for your chronic low back pain at our Gilbert, AZ clinic.
How Does PRP Compare to Cortisone and Radiofrequency Ablation for SI Joint Pain?
PRP differs from cortisone and radiofrequency ablation (RFA) for SI joint pain in a fundamental way: PRP targets the damaged ligaments and joint inflammation that drive the pain, while cortisone and RFA suppress symptoms without addressing the underlying cause. A lot of our patients have already tried cortisone by the time they reach us, and some have been offered RFA as the next step. PRP is the only one of the three that goes after the ligament damage directly, so the outcomes we see from properly dosed PRP tend to hold up in a way that cortisone and RFA do not.
Here is how the three most common injection-based treatments for SI joint pain compare on the factors that actually drive a decision:
| Factor | PRP | Cortisone (Steroid) | Radiofrequency Ablation |
|---|---|---|---|
| Mechanism | Concentrated growth factors delivered into damaged ligaments and the SI joint | Suppresses inflammation and numbs the pain signal | Burns the sensory nerves that transmit pain from the joint |
| Typical effect window | Gradual improvement over 4 weeks to 6 months; results can last >2 years | Days to a few months; often shorter with each repeat injection | 6 to 12 months, until the nerves regenerate and pain returns |
| Repeated use | Can be repeated, with improvements being additive | Can be repeated, but associated with tissue degradation and repeat treatments are typically less successful | Can be repeated when nerves regrow, but repeat treatments are typically less successful |
| Image guidance | Ultrasound-guided into the specific ligaments; ultrasound and x-ray guidance for the SI joint | Fluoroscopy; typically targets joint space only | Fluoroscopy; targets the lateral branch nerves |
| Key caveat | Off-label use in the US; results depend on accurate diagnosis and adequate platelet dose | Most useful short-term as a diagnostic tool or bridge, not a long-term plan | Best reserved for patients who can only work with insurance |
Cortisone may be useful early in the diagnostic process, specifically as an intra-articular block that helps confirm whether the SI joint is where the pain is coming from. The problem is that repeated cortisone for pain relief without a repair-oriented plan gives progressively shorter relief with each injection, and repeated steroid has been associated with connective tissue degradation in the orthopedic literature. Radiofrequency ablation can give meaningful relief in the right candidate, but it does not address the ligament laxity that often underlies SI joint dysfunction. When the nerves grow back in 6 to 12 months the pain typically returns, and subsequent treatments provide progressively shorter relief. PRP is the only one of the three that goes after what is actually wrong with the tissue.
What to Expect at Our Mesa-Area Clinic for SI Joint Pain
Your first visit is a 2-hour evaluation with hands-on testing for the low back, including the SI joint, combined with diagnostic ultrasound when indicated, before any treatment is recommended. Learn more about PRP therapy at our Mesa-area clinic.
This is not a quick consultation where you describe your symptoms and receive a prescription or an injection. We take a comprehensive approach to accurately identify the exact structures causing your pain before recommending any treatment.
Comprehensive 2-Hour Evaluation
Every new patient starts with a detailed 2-hour evaluation that includes a thorough history, hands-on physical examination with specific tests for SI joint instability and ligament laxity, plus diagnostic ultrasound when indicated. We test the SI joint and surrounding ligaments directly to determine whether they are the source of your pain, rather than relying solely on imaging.
The primary purpose of this evaluation is to identify the specific tissues causing your pain. This step is crucial because proper diagnosis is the single most important factor in regenerative treatment success.
Individualized Treatment Plan
Based on the evaluation, we determine whether you are a candidate for PRP injection or another regenerative approach. From there, we develop an orthobiologic plan specific to your case, including which structures will be treated, the expected timeline, and your role in recovery.
Because the first three months after a PRP injection are the critical window where most healing occurs, we typically recommend supplements and peptides to support the healing process. Our goal is to give your body every advantage during that healing window.
Ultrasound- and X-Ray-Guided PRP Injection
On your treatment day, we draw 120 to 300 mL of your blood, depending on how many structures we are treating. The preparation process typically takes one to one and a half hours because of how meticulous we are with processing. During this time, you relax in our IV lounge while we prepare your PRP to the highest standard.
The specific sacroiliac ligaments identified during the physical exam are treated under ultrasound guidance. The SI joint itself is treated under ultrasound and x-ray (fluoroscopic) guidance. We treat each structure individually rather than relying on a single intra-articular injection into the joint space.
Recovery and Follow-Up
After your injection, we recommend resting for the remainder of that day so your body can begin the healing process. Physical activity restrictions typically last 1 to 4 weeks, with a gradual return to full activity guided by your response. For most patients, we refer to a physical therapist who will design and adjust a rehabilitation plan specific to your treatment and goals.
In our clinic, most patients begin to notice changes within 4 weeks, with most of the improvement occurring over the first 3 months. Individual results may vary.
We schedule follow-up assessments to track your progress using our outcome registry, giving both you and our team objective data on how your treatment is working.
Schedule a comprehensive 2-hour evaluation for your chronic low back pain at our Gilbert, AZ clinic.
Who Is a Good Candidate for PRP SI Joint Treatment in Mesa, AZ?
PRP is typically a good fit for adults with chronic low back, hip, or leg pain that has not responded to physical therapy, pain medications, cortisone injections, or even surgery. Our 2-hour evaluation is designed to confirm whether the SI joint is the actual source for your specific situation.

Most patients who come to us share a similar profile. If you see yourself in the list below, PRP for SI joint pain may be worth exploring.
- Location: Mesa, Gilbert, Apache Junction, Chandler, or the greater Phoenix area
- Chronic low back pain for 3 months or longer that has not responded to disc-focused treatments
- Diagnosed with sciatica, a disc herniation, or degenerative disc disease, but treatments based on those diagnoses have not helped
- Pain worse with transitions: sitting to standing, getting in and out of the car, rolling over in bed
- Low back pain that radiates into the hip, buttock, groin, or down the leg
- Pain that started after pregnancy, a fall, or an accident
- Looking for a thorough evaluation that goes beyond an MRI and tests the SI joint and its supporting ligaments directly
- You are willing to invest in your health, as these are cash-pay procedures.
During your evaluation, we will assess whether PRP is the right approach for your specific condition, or whether a different regenerative treatment (such as nerve hydrodissection or autologous stem cell therapy) might be more appropriate.
If you are unsure whether orthobiologic injections like PRP or stem cell therapy are appropriate, or you are traveling from outside the Phoenix area, you can also call and ask about a brief 15 minute discovery call.
Frequently Asked Questions About PRP for SI Joint Pain
Can PRP help sacroiliac joint dysfunction?
PRP can help many patients with SI joint dysfunction by supporting tissue healing in the damaged and painful ligaments that stabilize the joint. Results are best when the diagnosis is accurate and the specific pain-generating structures are targeted under image guidance (ultrasound for the ligaments; ultrasound and x-ray for the joint itself).
In our registry, most lumbosacral and pelvis patients (which includes SI joint cases) report significant pain relief by 12 months, with relief largely holding through 18 months. Results vary, and not every case of SI joint dysfunction is a good fit for PRP.
How do I know if my low back pain is from the SI joint?
Pain with transitions, such as sitting to standing, getting in and out of the car, or rolling over in bed, is one of the most reliable clues that the SI joint may be involved. SI joint pain can also refer into the hip, groin, buttock, and down the leg, which is why it often gets mistaken for sciatica or a disc problem. A physical examination that specifically tests the SI joint, rather than just ordering an MRI, is the most accurate way to determine whether the SI joint is the source.
What does SI joint pain feel like and where is it located?
If you have SI joint pain, you usually feel it just below the belt line on one side, in the dimple area just inside the back of the pelvis, and it often refers into the buttock, hip, groin, or down the back of the thigh. Patients often describe it as a deep, sometimes constant ache that gets worse with sitting, stair climbing, rolling over in bed, or standing on one leg, and many patients have been told it was a disc problem or hip problem because of where it radiates.
SI joint pain can travel below the knee, but this is rare. This is one of the things that separates it from nerve root pain on a physical exam. It also tends to be one-sided, but it can still be on both sides, and reproducible with specific tests that load the joint. This is why a hands-on evaluation usually outperforms imaging in making this diagnosis.
What causes SI joint dysfunction?
SI joint dysfunction develops when the ligaments that stabilize the joint become lax, injured, or chronically irritated, and the most common triggers we see are pregnancy and childbirth, which puts hormonal laxity and mechanical stress on the joint at the same time, a fall or car accident that landed on the tailbone or the side of the pelvis, repeated impact activity, a prior lumbar fusion that shifted load to the SI joint, and gradual weakening over time with no single clear event.
In our Mesa-area patients we most often see two profiles: adults who had a specific injury years ago and a slow drift into chronic pain, and adults who cannot point to a single event but have had progressive pain that was worked up as a disc problem and never fully explained.
Is SI joint pain the same as sciatica?
SI joint pain and sciatica are different conditions, but they can produce similar symptoms, including pain that radiates down the leg. True sciatica involves compression of the sciatic nerve or its nerve roots, usually from a disc herniation. SI joint dysfunction involves the sacroiliac joint and its ligaments rather than the spinal nerve roots themselves. In our clinic, we regularly see patients who were diagnosed with sciatica but whose pain actually originates from the SI joint. When the joint is treated directly, the radiating leg pain often improves significantly.
How is SI joint pain diagnosed, and why isn't an MRI enough?
SI joint pain is mainly a clinical diagnosis, meaning it comes from a detailed physical exam using specific provocation tests, which are maneuvers like the FABER test, SI compression and distraction tests, thigh thrust test, and Gaenslen's test that load the SI joint and reproduce the patient's pain. A diagnostic intra-articular injection that temporarily relieves the pain can further confirm the source, although this is often not necessary if the physical exam is conclusive. An MRI is often completely normal in SI joint dysfunction, because the issue is often in the sacroiliac ligaments, which don't show up clearly on standard imaging.
This is often a real source of frustration for a lot of our patients, because they come in with a clean MRI and a history of "everything looks fine" from their primary care or orthopedist, and the pain is still there. A properly trained physical exam and diagnostic ultrasound evaluation usually identifies what imaging alone missed.
How does PRP work for SI joint pain?
PRP for SI joint pain uses platelets and growth factors concentrated from your own blood to support repair in the sacroiliac ligaments and joint. Under ultrasound guidance, PRP is injected directly into the sacroiliac ligaments that are lax or damaged, and then under ultrasound and x-ray guidance, PRP is injected directly into the joint.
See the full breakdown in the How PRP Injections Work section above.
How many PRP treatments does SI joint dysfunction require?
We start with one PRP injection and track your individual response over a 3-month period. A second treatment may be indicated, based on your response after the 3 months. Each visit is guided by a new physical examination, not simply a fixed protocol schedule.
How long can PRP results for SI joint pain last?
Many patients experience lasting improvement after PRP treatment for SI joint dysfunction, especially when ligament laxity is accurately identified and treated. DataBiologics data from Regenerative Performance show most patients report continued relief through 18 months of follow-up. Individual results vary depending on the severity of the condition, activity level, and overall health.
What is the success rate of PRP for SI joint pain?
Published research on PRP for the SI joint is still early, but what exists is promising. In a 2017 randomized trial by Singla and colleagues comparing ultrasound-guided PRP to steroid injection for chronic SI joint pain, 90% of PRP patients maintained significant pain relief at 3 months compared to 25% of steroid patients, and PRP patients were 37 times more likely to achieve at least 50% pain reduction. These numbers reflect what we see in our clinic when the diagnosis is right and the dose is right.
In our patient outcome registry, lumbosacral and pelvis cases (which include sacroiliac joint dysfunction along with other low back and pelvic pain generators) show 74% of patients reporting significant pain relief at 12 months, and 77% reporting relief at 18 months.
Is PRP for SI joint pain safe, and what are the side effects?
PRP comes from your own blood, so the risk of allergic reaction or transmitted infection is very low. The most common side effects are soreness, bruising, and a temporary flare in pain at the injection site for 2 to 5 days after treatment, which is the intended inflammatory repair response and not a sign that something went wrong.
Serious complications are rare when injections are image-guided (ultrasound and/or x-ray) by a clinician trained in MSK interventional procedures.
PRP vs cortisone for SI joint pain: which is better?
Cortisone can give short-term relief, and it can also be a useful diagnostic tool when placed into the joint under imaging guidance, which can help confirm whether the SI joint is where the pain is coming from. But, the problem with cortisone as a long-term plan is that it does not address the ligament damage that usually underlies chronic SI joint pain, so the relief gets shorter with each round. Repeated cortisone injections have been shown to accelerate cartilage breakdown in the knee (McAlindon et al., JAMA, 2017), and this may be true for other joints such as the SI joint.
PRP targets those structures directly, so the outcomes we see from properly dosed, image-guided PRP tend to hold up in a way that cortisone does not. For the full side-by-side, see the How Does PRP Compare to Cortisone and Radiofrequency Ablation section above.
Still have questions? The best way to get answers is a conversation. Call 480-508-4226.

About Dr. Drew Timmermans
Dr. Drew Timmermans, ND, RMSK, specializes in precision-guided orthobiologic injections for chronic musculoskeletal pain. He has extensive experience evaluating and treating sacroiliac joint dysfunction, which is significantly underdiagnosed in the conventional medical care system.
Every patient receives a full 2-hour evaluation with hands-on physical examination and diagnostic ultrasound to identify the specific tissues generating pain. Regenerative Performance is located in Gilbert, AZ, and serves patients across the greater Phoenix area.
References
- Sembrano JN, Polly DW. How often is low back pain not coming from the back? Spine. 2009;34(1):E27-E32. doi:10.1097/BRS.0b013e31818b8882
- Cohen SP, Chen Y, Neufeld NJ. Sacroiliac joint pain: a comprehensive review of epidemiology, diagnosis, and treatment. Expert Rev Neurother. 2013;13(1):99-116. doi:10.1586/ern.12.148
- Singla V, Batra YK, Bharti N, Goni VG, Marwaha N. Steroid vs. Platelet-Rich Plasma in Ultrasound-Guided Sacroiliac Joint Injection for Chronic Low Back Pain. Pain Pract. 2017;17(6):782-791. doi:10.1111/papr.12526
- McAlindon TE, LaValley MP, Harvey WF, et al. Effect of Intra-articular Triamcinolone vs Saline on Knee Cartilage Volume and Pain in Patients With Knee Osteoarthritis: A Randomized Clinical Trial. JAMA. 2017;317(19):1967-1975. doi:10.1001/jama.2017.5283
NOTE: This article provides general information to help the reader better understand regenerative medicine, nerve and musculoskeletal conditions, naturopathic approaches to pain, and related subjects. All content provided in this article, website, or any linked materials, including text, graphics, images, research, and outcomes, are not intended, and should not be used, as a substitute for direct medical advice, diagnosis, or treatment. Please always consult with a professional and licensed healthcare provider to discuss if any treatment is right for you.
Registry data from our single practice, powered by DataBiologics, is not a randomized clinical trial. Individual results may vary.